
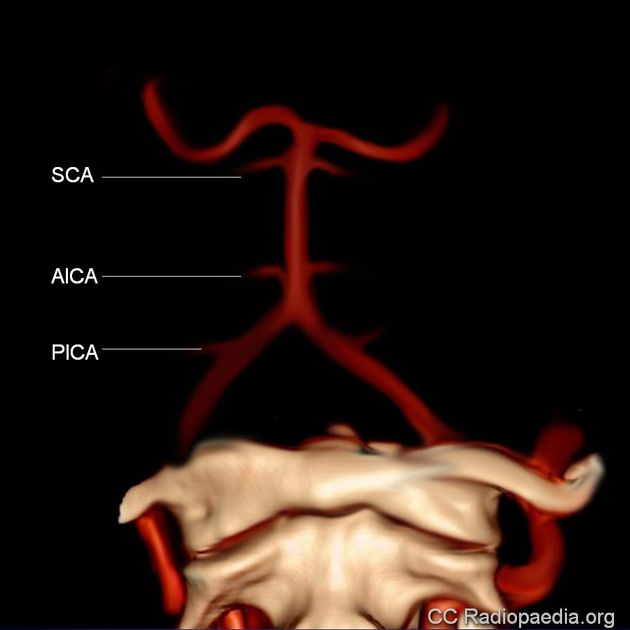
Anterior inferior cerebellar artery (AICA) territory infarcts are a rare cause of cerebellar strokes. AICA strokes are much less common than posterior inferior cerebellar artery (PICA) infarcts. AICA generally arises from the caudal third of the basilar artery and supplies the lateral pons, inner ear, middle cerebellar peduncle and the anterior inferior cerebellum 4,5.
On this page:
Epidemiology
AICA territory infarcts are rare, comprising ~1% of ischemic strokes 2.
Clinical presentation
Vertigo (can be central or peripheral due to the arterial supply) is the most common symptom associated with an AICA infarct, however, it is normally associated with neurological signs and symptoms such as ipsilateral hypoacusis (hearing loss), facial weakness, facial sensory loss, crossed body sensory loss, gait ataxia, limb ataxia and Horner syndrome 4-7.
Pathology
Acute interruption of blood flow through the AICA which leads to deprivation of oxygen and glucose in the vascular territory supplied. This phenomenon triggers a cascade of events at a cellular level, that if the circulation is not restored in time, will lead to cell death.
The main cause of AICA territory stroke is atherosclerosis, but can also be a lacunar infarct due to thromboembolism, although sometimes the cause is not known.
Radiographic features
Generally, the features are those of ischemic stroke in the anterior cerebellar artery vascular territory, including the middle cerebellar peduncle, inferolateral portion of the pons, flocculus, and anteroinferior surface of the cerebellum.
For detailed discussion, see: ischemic stroke.





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.