
Anterior suprapatellar (quadriceps) fat pad impingement syndrome is a controversial cause of anterior knee pain although anterior suprapatellar fat pad oedema may often, and possibly more commonly, be incidental or considered an anatomical variant 1,2,11.
On this page:
Clinical presentation
Patients present with anterior knee pain and with the point of tenderness at the superior pole of the patella. The pain is exacerbated on deep knee flexion.
Pathology
Aetiology
The aetiology is unclear. It is suggested to result from repeated microtrauma resulting in fibrosis and haemorrhage. There is no significant correlation with patellofemoral maltracking 8. There is an association with patellofemoral joint degeneration 9.
Radiographic features
MRI
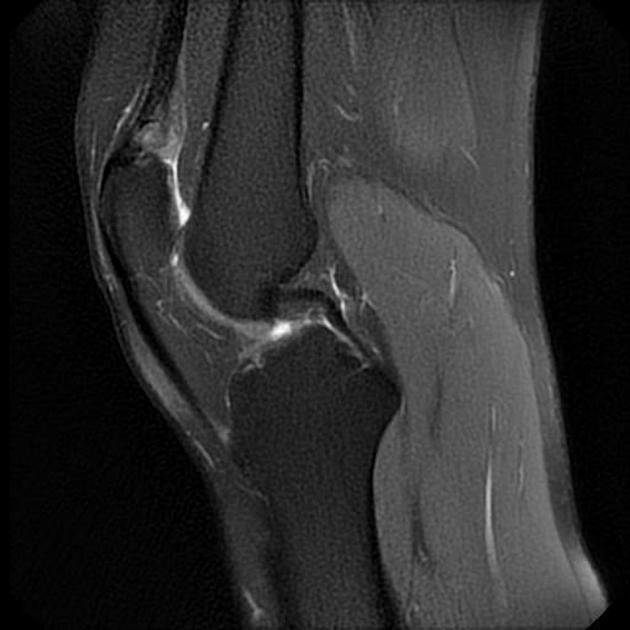
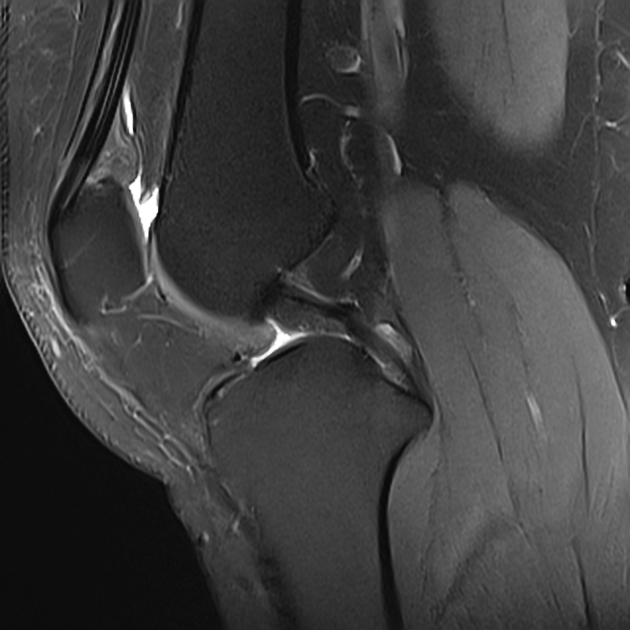
The anterior suprapatellar fat pad is oedematous compared to the prefemoral fat pad, enlarged (≥10 mm AP diameter) with a mass effect on the adjacent suprapatellar recess (i.e. a convex border) and quadriceps tendon 1-4.
T1: low signal within the suprapatellar fat pad
T2: high signal within the suprapatellar fat pad
T1 C+ (Gd): enhancement of the suprapatellar fat pad
The most common associated MRI findings are joint effusion and quadriceps tendinitis 10.
Treatment and prognosis
Initial management is usually conservative, like anti-inflammatory medications and decreased painful activities. Complete pain resolution can be achieved with ultrasound-guided injection of anaesthetic or corticosteroid followed by physical therapy 6. Surgery could be considered in cases with persistent symptoms by laparoscopic resection 7.
Differential diagnosis
In the absence of anterior knee pain, quadriceps fat pad oedema diagnosis cannot be made based solely on MRI findings 1,2.










 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.