
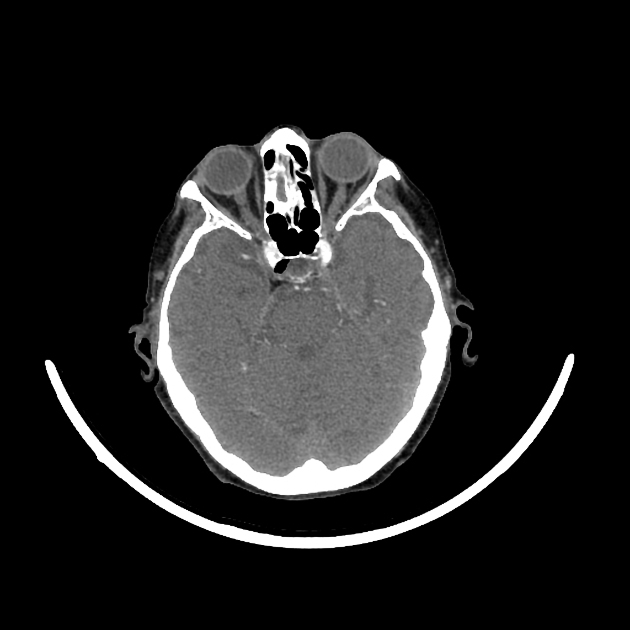
Cavernous sinus gas locules can be seen in several settings.
iatrogenic pneumocephalus secondary to gas embolism (especially venous gas embolism) from IV access (can be a relatively common finding in the absence of direct trauma and does not usually require treatment)
traumatic pneumocephalus: in the context of trauma, sphenoid or skull base fracture needs to be excluded in this context
barotrauma
very rarely infection from a gas-forming organism
Practical points
Any intravenous injectate administered into the upper extremity normally travels through the axillary, subclavian, and brachiocephalic veins to empty into the superior vena cava. However, under certain clinical circumstances such as stenosis of the brachiocephalic vein/SVC, heart failure, coughing etc. it flows cephalad through the internal and external jugular veins into the cranial venous system.
Additionally, air locules are lighter than blood, therefore can rise retrogradely up through the jugular veins, especially in patients who are in a reclining position. Air bubbles thus accumulate in the highest areas of the head, especially in the cavernous sinuses, the frontal venous system, petrosal sinuses, superficial temporal veins, and orbital veins.




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.