
Cystic nephromas, previously known as multilocular cystic nephromas, are rare benign renal neoplasms classically occurring in adult females in the 4th and 5th decades. As of the 2016 WHO classification, they are considered distinct from pediatric cystic nephromas which have associated DICER1 gene mutation 10,11,14.
On this page:
Terminology
Evolving terminology regarding cystic nephromas and other cystic renal tumors reflects ongoing changes in classification, in step with shifting understanding of the disease processes and genetic aberrations.
Classically, cystic nephromas were thought to occur in a bimodal age distribution, affecting young children and adults in middle age and the generic term "multilocular cystic renal tumor" was sometimes used.
Lesions arising in children are distinct from adult cystic nephromas on both immunohistochemical and genetic bases, and are separately categorized by WHO 10,11,14.
cystic nephroma (adult)
pediatric cystic nephroma (pediatric)
cystic partially differentiated nephroblastoma (pediatric)
As of 2016, the WHO classifies cystic nephroma within the mixed epithelial and stromal tumor (MEST) family along a spectrum of disease 10,13,14. The remainder of this article will discuss the adult form of cystic nephroma.
Epidemiology
The condition is rare, and occurs most commonly in female adults (50-60 years) and pediatric males.
Clinical presentation
Patients usually present with abdominal pain and a palpable abdominal mass 12, however some cases may be asymptomatic and incidentally discovered on imaging.
Pathology
Grossly, multilocular cystic renal tumors are typically unifocal multiloculated cystic masses surrounded by a thick fibrous capsule and compressed parenchyma 8. Calcification, hemorrhage, and necrosis are unusual.
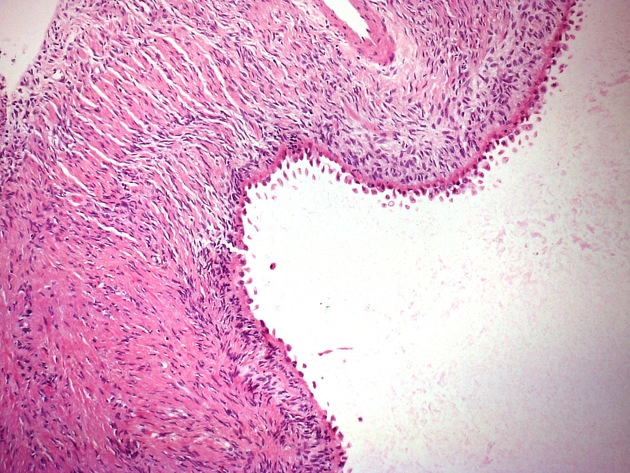
Microscopically, these tumors are lined by flat, cuboid, or hobnail cells 8, while the fibrous septa may contain mature tubules 3.
Radiographic features
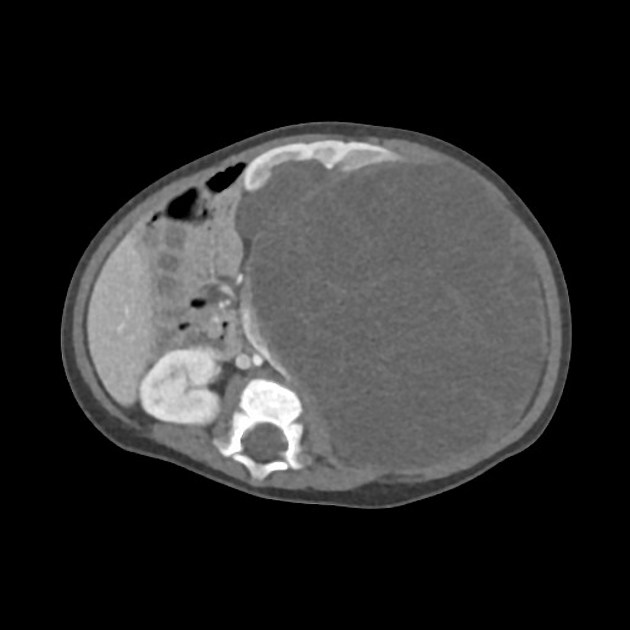
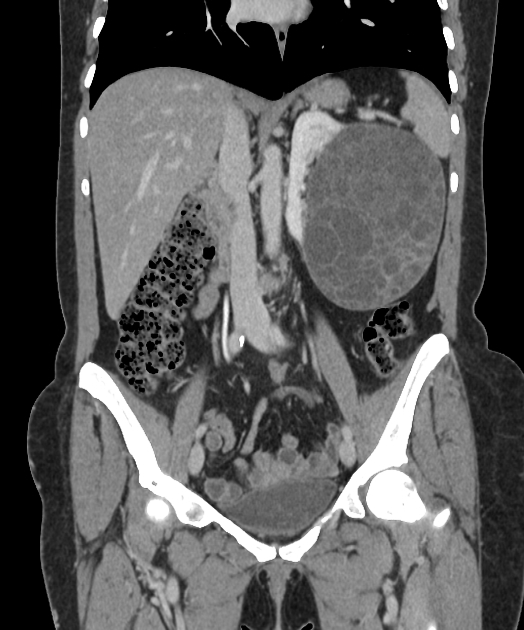
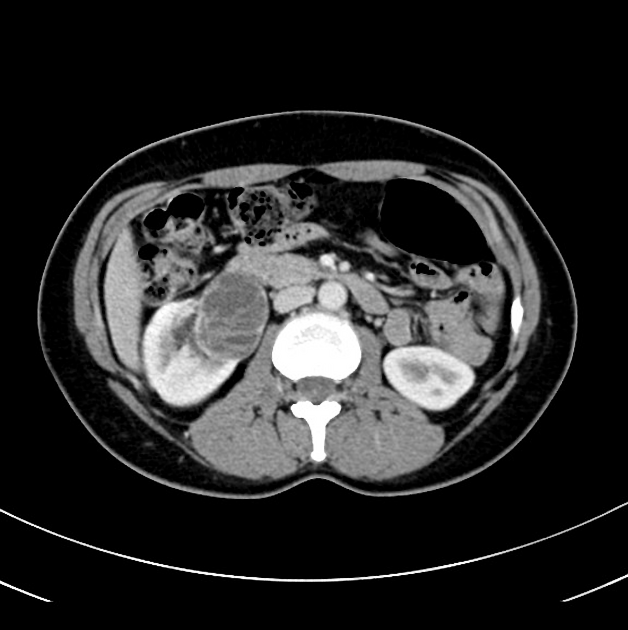
Multilocular cystic renal tumors generally have the appearance of a multilocular cystic encapsulated mass on most modalities.
Plain radiograph
May present as a large abdominal mass displacing and effacing adjacent bowel loops.
Ultrasound
-
multilocular cystic mass originating from kidney 4
claw or beak-shape of adjacent renal parenchyma (claw sign) may help confirm a renal origin
cyst contents usually anechoic, but low-level echoes may be seen
septal vascularity can also be seen 8
CT
multilocular cystic mass often herniates into the renal pelvis causing a filling defect and sometimes obstructive calycectasis
variable septal enhancement
no nodular or solid enhancement 8
+/- associated streakiness in perirenal fat 4
excretion of contrast by the affected kidney is usually normal
MRI
Signal characteristics include:
T1: variable signal, depending on the protein or blood products of the cysts
T2: hyperintense (cysts)
T1 C+ (Gd): septal enhancement may be seen
Treatment and prognosis
Radical or partial nephrectomy is usually done, with lymph node excision.
Differential diagnosis
Cystic nephroma is indistinguishable from multilocular cystic renal neoplasm of low malignant potential, formerly multilocular cystic renal cell carcinoma 15.





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.