
Desmoid tumours are benign, non-inflammatory fibroblastic tumours with a tendency for local invasion and recurrence post resection. They are sometimes considered a locally aggressive proliferative disease within the family of soft-tissue sarcomas but, metastasis is uncommon 7,11.
On this page:
Terminology
The terms desmoid tumour and aggressive fibromatosis are occasionally used synonymously by some authors 9. This article will focus on the abdominal presentation of this fibroblastic tumour. For the musculoskeletal presentation, please refer to the latter.
Epidemiology
They are rare tumours, thought to account for only ~0.03% of all neoplasms 6. Desmoid tumours are found in all age groups but are most frequently encountered between 20 and 40 years of age. They are seen more in women (2:1). They are rare lesions with an estimated incidence of 3.7 new cases per million population per year 1.
Associations
some cases have been associated with pregnancy and oestrogen therapy 10
in the case of mesenteric desmoid they are seen either sporadically or in association with familial polyposis coli syndrome (FAP): 9-18% of FAP cases may have a desmoid tumour 8
Clinical presentation
Desmoid tumours present as masses, and as such presentation depends on location.
Pathology
Their exact aetiology remains uncertain, although they are frequently associated with previous trauma or surgical incision. On the molecular level, desmoids are characterised by mutations in the β-catenin gene, CTNNB1, or the adenomatous polyposis coli (APC) gene 7.
Location
Frequent locations in the abdomen are the abdominal wall, the root of the mesentery and the retroperitoneum.
Classification
Desmoid-type fibromatosis is listed in the WHO classification of soft tissue tumours under the category "fibroblastic/myofibroblastic tumours".
Radiographic features
Ultrasound
Desmoid tumours are the commonest neoplasms of the abdominal wall and typically appear as homogeneously hypoechoic masses. They may have a similar appearance to muscle, may be lobulated and may show vascularity on colour Doppler interrogation.
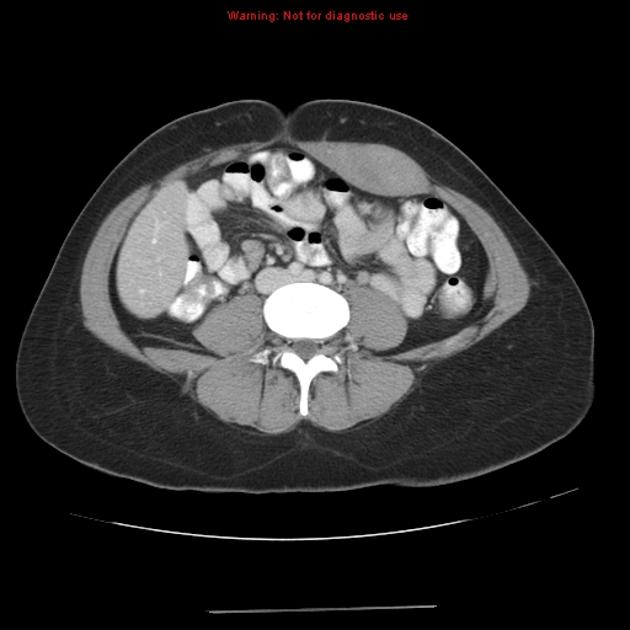
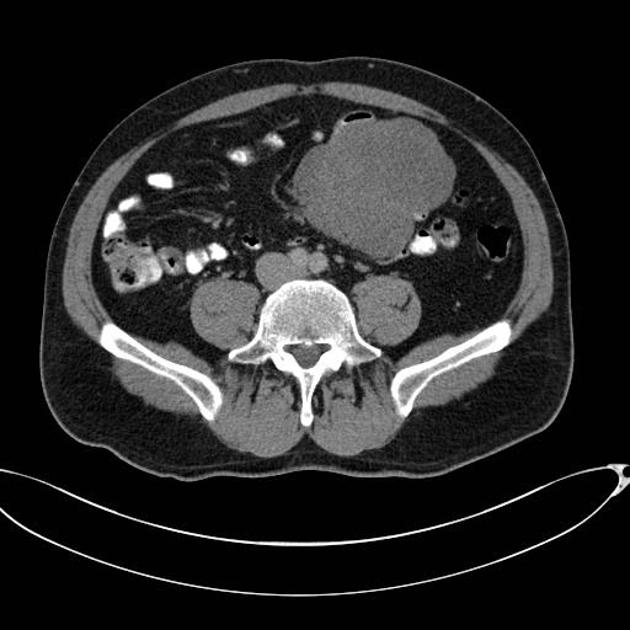
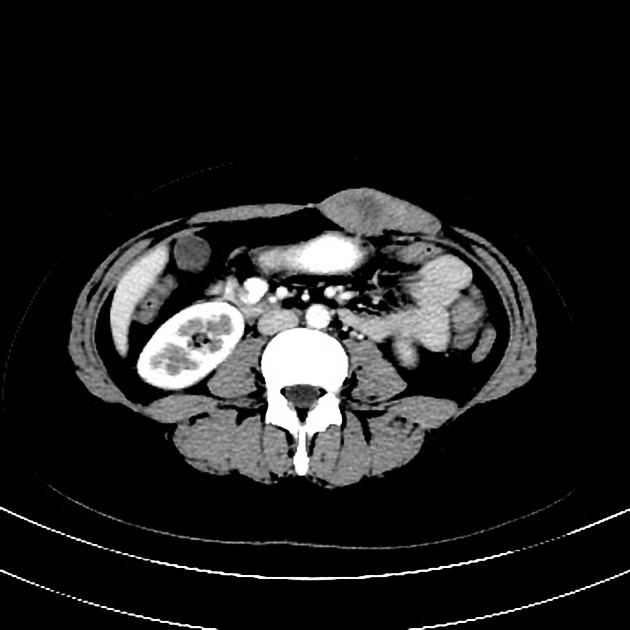
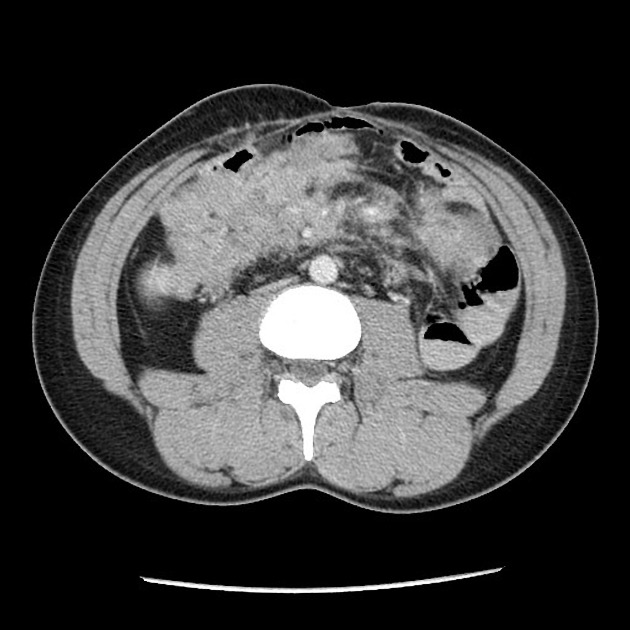
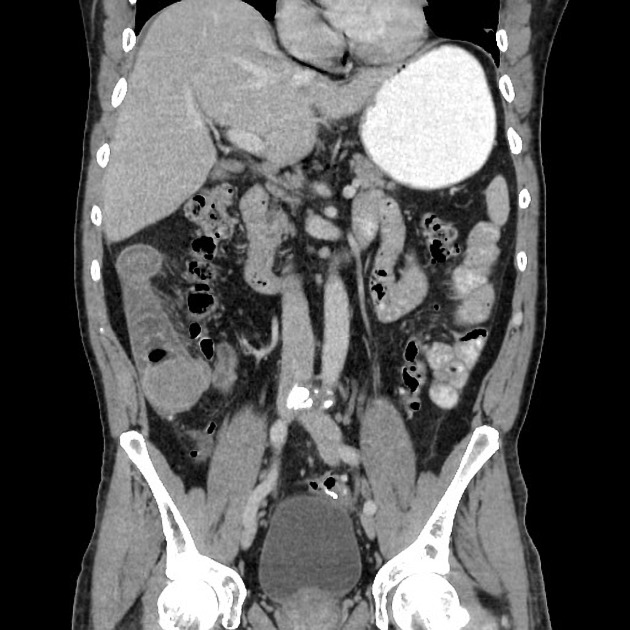
CT
most desmoid tumours are well-circumscribed masses, although in some cases they may appear more aggressive with ill-defined margins
most are relatively homogeneously or focally hyperattenuating when compared to soft tissue on the non-contrast scan
most will demonstrate enhancement following administration of intravenous contrast
MRI
MRI, as is the case with other soft tissue tumours, is more sensitive to local tumour extension. Their appearance is accounted for by their dense cellularity. Typical signal characteristics include:
T1: low signal intensity
T2: low signal intensity
T1 C+ (Gd): may show homogeneous, inhomogeneous, or no significant enhancement 8
Treatment and prognosis
Most cases can have relatively good prognosis and watchful waiting is now considered a reasonable option in selected asymptomatic patients 7. Other management options include ref:
-
surgical resection (traditionally used, although recurrence rate is high)
NSAIDs and anti-oestrogens can be used to reduce the rate of recurrence
Differential diagnosis
sclerosing mesenteritis: tends to be more central at the "root" of the mesentery ref
History and etymology
The term "desmoid" originates from the Greek word "desmos" (Δεσμός’) meaning band or tendon-like.




















 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.