Graves disease
Updates to Article Attributes
Graves disease,also known as Basedow disease inmainland Europe9, is an autoimmune thyroid disease and is the most common cause of hyperthyroidism.
Epidemiology
There is a strong female predilection (F:M of 5:1), and is most common between 30 and 60 years 14. The incidence is 20 cases per 100,000 people 14.
Paediatric Graves disease accounts for 5% of all cases (incidence 5 per 100,000 children). It is more common in older adolescents. There is a lower female prediction in children (F;M of 3.5:1) 15.
Clinical presentation
Patients are thyrotoxic with common symptoms being tremor, heat sensitivity, unexplained weight loss, anxiety, goitre, etc. 14. Extrathyroidal manifestations include:
- Graves ophthalmopathy (orbitopathy): affects 20-25% of cases
- thyroid dermopathy (formerly called pretibial myxoedema): occurs in ~2% and is almost always associated with thyroid ophthalmopathy 7
- thyroid acropachy: occurs in ~1% 7
- encephalopathy associated with autoimmune thyroid disease (EAATD) 2,8:much more commonly associated with Hashimoto thyroiditis
The combination of exophthalmos, palpitations, and goitre is called the Merseburger (or Merseburg) triad.
Pathology
Graves disease results from an antibody-directed stimulation of the thyroid-stimulating hormone (TSH) receptor, with the production and release of T3 and T4 resulting in hyperthyroidism 14.
Aetiology
The pathogenesis of Graves disease is not fully known 15. Genetic predisposition accounts for 80% of the risk of Graves disease, with environmental factors (e.g. smoking, iodine excess, selenium deficiency, vitamin D deficiency) accounting for the rest 14.
Macroscopic appearance
The affected gland shows diffuse, symmetrical enlargement, with a fleshy red cut surface. This appearance can be altered by preoperative treatment or chronicity.
Microscopic appearance
The histological features are consistent with the activated state of the gland:
- plump follicular cells with increased amounts of eosinophilic cytoplasm
- hyperplastic follicles with papillary epithelial infoldings
- evidence of colloid reabsorption, including 'scalloping' at the apical membrane and variable follicle collapse and exhaustion
These features can be altered by preoperative treatment or chronicity.
Serology
- TSH: suppressed
- T4: elevated
- T3: elevated
- TSH receptor antibodies (TSI, TGI, TBII): positive
Associations
10x increased relative risk of the following autoimmune diseases 16:
- rheumatoid arthritis (most common co-existing autoimmune disorder)
- pernicious anaemia
- systemic lupus erythematosus
- Addison disease
- coeliac disease
- vitiligo
Radiographic features
Ultrasound
- thyroid gland is often enlarged and can be hyperechoic
- heterogeneous thyroid echotexture
- relative absence of nodularity in uncomplicated cases
- hypervascular; may demonstrate a thyroid inferno pattern on colour Doppler 1
Nuclear medicine
- iodine-123: imaging performed at around 2-6 days; classically demonstrates homogeneously increased activity in an enlarged gland
- technetium-99m pertechnetate: homogeneously increased activity in an enlarged thyroid gland
Treatment and prognosis
Antithyroid medications (e.g. methimazole/carbimazole) are the first-line treatment. In medication-resistant Graves disease, patients can go onto radioactive iodine or thyroidectomy 14,15.
Complications
- increased risk of thyroid cancer 14
History and etymology
It is named after Robert James Graves (1796-1852), an Irish surgeon who first described it in 1835 9, and Carl Adolph von Basedow (1799-1854), a German physician who described it in 1840 10,11,13. The Merseburger triad was first described by Basedow, who practised in Merseburg 12,13.
Differential diagnosis
For hyperthyroidism consider:
- Marine-Lenhart syndrome
- toxic thyroid adenoma
- toxic multinodular goitre
- inflammatory
- pituitary adenoma
- extrathyroid origin
- struma ovarii
- metastatic thyroid carcinoma
- factitious hyperthyroidism
Practical points
- patients with Graves disease are at higher risk of iodinated contrast media-induced thyrotoxicosis
-<p><strong>Graves disease</strong>,<strong> </strong>also known as <strong>Basedow disease </strong>in<strong> </strong>mainland Europe<strong> </strong><sup>9</sup>, is an <a href="/articles/autoimmune-thyroid-disease">autoimmune thyroid disease</a> and is the most common cause of <a href="/articles/hyperthyroidism">hyperthyroidism</a>.</p><h4>Epidemiology</h4><p>There is a strong female predilection (F:M of 5:1), and is most common between 30 and 60 years <sup>14</sup>. The incidence is 20 cases per 100,000 people <sup>14</sup>.</p><p>Paediatric Graves disease accounts for 5% of all cases (incidence 5 per 100,000 children). It is more common in older adolescents. There is a lower female prediction in children (F;M of 3.5:1) <sup>15</sup>.</p><h4>Clinical presentation</h4><p>Patients are thyrotoxic with common symptoms being tremor, heat sensitivity, unexplained weight loss, anxiety, <a href="/articles/goitre-2">goitre</a>, etc. <sup>14</sup>. Extrathyroidal manifestations include:</p><ul>-<li>-<a href="/articles/graves-ophthalmopathy">Graves ophthalmopathy</a> (orbitopathy): affects 20-25% of cases</li>-<li>-<a href="/articles/thyroid-dermopathy">thyroid dermopathy</a> (formerly called pretibial myxoedema): occurs in ~2% and is almost always associated with thyroid ophthalmopathy <sup>7</sup>-</li>-<li>-<a href="/articles/thyroid-acropachy">thyroid acropachy</a>: occurs in ~1% <sup>7</sup>-</li>-<li>-<a href="/articles/steroid-responsive-encephalopathy-associated-with-autoimmune-thyroiditis-1">encephalopathy associated with autoimmune thyroid disease (EAATD)</a> <sup>2,8</sup>:<a href="/articles/steroid-responsive-encephalopathy-associated-with-autoimmune-thyroiditis-1"></a>much more commonly associated with <a href="/articles/hashimoto-thyroiditis">Hashimoto thyroiditis</a>-</li>-</ul><p>The combination of exophthalmos, palpitations, and goitre is called the Merseburger (or Merseburg) triad.</p><h4>Pathology</h4><p>Graves disease results from an antibody-directed stimulation of the thyroid-stimulating hormone (TSH) receptor, with the production and release of T3 and T4 resulting in <a href="/articles/hyperthyroidism">hyperthyroidism</a> <sup>14</sup>.</p><h5>Aetiology</h5><p>The pathogenesis of Graves disease is not fully known <sup>15</sup>. Genetic predisposition accounts for 80% of the risk of Graves disease, with environmental factors (e.g. smoking, iodine excess, selenium deficiency, vitamin D deficiency) accounting for the rest <sup>14</sup>.</p><h5>Macroscopic appearance</h5><p>The affected gland shows diffuse, symmetrical enlargement, with a fleshy red cut surface. This appearance can be altered by preoperative treatment or chronicity.</p><h5>Microscopic appearance</h5><p>The histological features are consistent with the activated state of the gland:</p><ul>-<li>plump follicular cells with increased amounts of eosinophilic cytoplasm</li>-<li>hyperplastic follicles with papillary epithelial infoldings</li>-<li>evidence of colloid reabsorption, including 'scalloping' at the apical membrane and variable follicle collapse and exhaustion</li>-</ul><p>These features can be altered by preoperative treatment or chronicity. </p><h5>Serology</h5><ul>-<li>TSH: suppressed</li>-<li>T4: elevated</li>-<li>T3: elevated</li>-<li>TSH receptor antibodies (TSI, TGI, TBII): positive</li>-</ul><h5>Associations</h5><p>10x increased relative risk of the following autoimmune diseases <sup>16</sup>:</p><ul>-<li>-<a href="/articles/rheumatoid-arthritis">rheumatoid arthritis</a> (most common co-existing autoimmune disorder)</li>-<li><a href="/articles/pernicious-anaemia">pernicious anaemia</a></li>-<li><a href="/articles/systemic-lupus-erythematosus">systemic lupus erythematosus</a></li>-<li><a href="/articles/adrenal-insufficiency-1">Addison disease</a></li>-<li><a href="/articles/coeliac-disease-1">coeliac disease</a></li>-<li>vitiligo</li>-</ul><h4>Radiographic features</h4><h5>Ultrasound</h5><ul>-<li>thyroid gland is often enlarged and can be hyperechoic</li>-<li>heterogeneous thyroid echotexture</li>-<li>relative absence of nodularity in uncomplicated cases</li>-<li>hypervascular; may demonstrate a <a href="/articles/thyroid-inferno">thyroid inferno</a> pattern on colour Doppler <sup>1</sup>-</li>-</ul><h5>Nuclear medicine</h5><ul>-<li>-<a href="/articles/iodine-123">iodine-123</a>: imaging performed at around 2-6 days; classically demonstrates homogeneously increased activity in an enlarged gland</li>-<li>-<a href="/articles/tc-99m-pertechnetate">technetium-99m pertechnetate</a>: homogeneously increased activity in an enlarged thyroid gland</li>-</ul><h4>Treatment and prognosis</h4><p>Antithyroid medications (e.g. methimazole/carbimazole) are the first-line treatment. In medication-resistant Graves disease, patients can go onto radioactive iodine or thyroidectomy <sup>14,15</sup>.</p><h5>Complications</h5><ul><li>increased risk of <a href="/articles/thyroid-malignancies">thyroid cancer</a> <sup>14</sup>-</li></ul><h4>History and etymology</h4><p>It is named after <strong>Robert James Graves </strong>(1796-1852),<strong> an </strong>Irish surgeon who first described it in 1835 <sup>9</sup>, and Carl Adolph von Basedow (1799-1854), a German physician who described it in 1840 <sup>10,11,13</sup>. The Merseburger triad was first described by Basedow, who practised in Merseburg <sup>12,13</sup>.</p><h4>Differential diagnosis</h4><p>For <a href="/articles/hyperthyroidism">hyperthyroidism</a> consider: </p><ul>-<li><a href="/articles/marine-lenhart-syndrome-3">Marine-Lenhart syndrome</a></li>-<li>toxic <a href="/articles/thyroid-adenoma">thyroid adenoma</a>-</li>-<li>toxic <a href="/articles/multinodular-goitre">multinodular goitre</a>-</li>-<li>-<a href="/articles/thyroid-inflammatory-conditions">inflammatory</a><ul>-<li><a href="/articles/de-quervain-thyroiditis">subacute thyroiditis</a></li>-<li><a href="/articles/postpartum-thyroiditis-2">postpartum thyroiditis </a></li>-<li><a href="/articles/subacute-lymphocytic-thyroiditis">silent thyroiditis</a></li>-</ul>-</li>-<li>-<a href="/articles/pituitary-adenomapitnet">pituitary adenoma</a> </li>-<li>extrathyroid origin</li>-<li><a href="/articles/struma-ovarii-tumour">struma ovarii</a></li>-<li><a href="/articles/metastatic-thyroid-carcinoma">metastatic thyroid carcinoma </a></li>-<li><a href="/articles/factitious-hyperthyroidism">factitious hyperthyroidism</a></li>-</ul><h4>Practical points</h4><ul><li>patients with Graves disease are at higher risk of <a href="/articles/iodinated-contrast-induced-thyrotoxicosis">iodinated contrast media-induced thyrotoxicosis</a>- +<p><strong>Graves disease</strong>,<strong> </strong>also known as <strong>Basedow disease </strong>in<strong> </strong>mainland Europe<strong> </strong><sup>9</sup>, is an <a href="/articles/autoimmune-thyroid-disease">autoimmune thyroid disease</a> and is the most common cause of <a href="/articles/hyperthyroidism">hyperthyroidism</a>.</p><h4>Epidemiology</h4><p>There is a strong female predilection (F:M of 5:1), and is most common between 30 and 60 years <sup>14</sup>. The incidence is 20 cases per 100,000 people <sup>14</sup>.</p><p>Paediatric Graves disease accounts for 5% of all cases (incidence 5 per 100,000 children). It is more common in older adolescents. There is a lower female prediction in children (F;M of 3.5:1) <sup>15</sup>.</p><h4>Clinical presentation</h4><p>Patients are thyrotoxic with common symptoms being tremor, heat sensitivity, unexplained weight loss, anxiety, <a href="/articles/goitre-2">goitre</a>, etc. <sup>14</sup>. Extrathyroidal manifestations include:</p><ul>
- +<li>
- +<a href="/articles/graves-ophthalmopathy">Graves ophthalmopathy</a> (orbitopathy): affects 20-25% of cases</li>
- +<li>
- +<a href="/articles/thyroid-dermopathy">thyroid dermopathy</a> (formerly called pretibial myxoedema): occurs in ~2% and is almost always associated with thyroid ophthalmopathy <sup>7</sup>
- +</li>
- +<li>
- +<a href="/articles/thyroid-acropachy">thyroid acropachy</a>: occurs in ~1% <sup>7</sup>
- +</li>
- +<li>
- +<a href="/articles/steroid-responsive-encephalopathy-associated-with-autoimmune-thyroiditis-1">encephalopathy associated with autoimmune thyroid disease (EAATD)</a> <sup>2,8</sup>:<a href="/articles/steroid-responsive-encephalopathy-associated-with-autoimmune-thyroiditis-1"></a>much more commonly associated with <a href="/articles/hashimoto-thyroiditis">Hashimoto thyroiditis</a>
- +</li>
- +</ul><p>The combination of exophthalmos, palpitations, and goitre is called the Merseburger (or Merseburg) triad.</p><h4>Pathology</h4><p>Graves disease results from an antibody-directed stimulation of the thyroid-stimulating hormone (TSH) receptor, with the production and release of T3 and T4 resulting in <a href="/articles/hyperthyroidism">hyperthyroidism</a> <sup>14</sup>.</p><h5>Aetiology</h5><p>The pathogenesis of Graves disease is not fully known <sup>15</sup>. Genetic predisposition accounts for 80% of the risk of Graves disease, with environmental factors (e.g. smoking, iodine excess, selenium deficiency, vitamin D deficiency) accounting for the rest <sup>14</sup>.</p><h5>Macroscopic appearance</h5><p>The affected gland shows diffuse, symmetrical enlargement, with a fleshy red cut surface. This appearance can be altered by preoperative treatment or chronicity.</p><h5>Microscopic appearance</h5><p>The histological features are consistent with the activated state of the gland:</p><ul>
- +<li>plump follicular cells with increased amounts of eosinophilic cytoplasm</li>
- +<li>hyperplastic follicles with papillary epithelial infoldings</li>
- +<li>evidence of colloid reabsorption, including 'scalloping' at the apical membrane and variable follicle collapse and exhaustion</li>
- +</ul><p>These features can be altered by preoperative treatment or chronicity. </p><h5>Serology</h5><ul>
- +<li>TSH: suppressed</li>
- +<li>T4: elevated</li>
- +<li>T3: elevated</li>
- +<li>TSH receptor antibodies (TSI, TGI, TBII): positive</li>
- +</ul><h5>Associations</h5><p>10x increased relative risk of the following autoimmune diseases <sup>16</sup>:</p><ul>
- +<li>
- +<a href="/articles/rheumatoid-arthritis">rheumatoid arthritis</a> (most common co-existing autoimmune disorder)</li>
- +<li><a href="/articles/pernicious-anaemia">pernicious anaemia</a></li>
- +<li><a href="/articles/systemic-lupus-erythematosus">systemic lupus erythematosus</a></li>
- +<li><a href="/articles/adrenal-insufficiency-1">Addison disease</a></li>
- +<li><a href="/articles/coeliac-disease-1">coeliac disease</a></li>
- +<li>vitiligo</li>
- +</ul><h4>Radiographic features</h4><h5>Ultrasound</h5><ul>
- +<li>thyroid gland is often enlarged and can be hyperechoic</li>
- +<li>heterogeneous thyroid echotexture</li>
- +<li>relative absence of nodularity in uncomplicated cases</li>
- +<li>hypervascular; may demonstrate a <a href="/articles/thyroid-inferno">thyroid inferno</a> pattern on colour Doppler <sup>1</sup>
- +</li>
- +</ul><h5>Nuclear medicine</h5><ul>
- +<li>
- +<a href="/articles/iodine-123">iodine-123</a>: imaging performed at around 2-6 days; classically demonstrates homogeneously increased activity in an enlarged gland</li>
- +<li>
- +<a href="/articles/tc-99m-pertechnetate">technetium-99m pertechnetate</a>: homogeneously increased activity in an enlarged thyroid gland</li>
- +</ul><h4>Treatment and prognosis</h4><p>Antithyroid medications (e.g. methimazole/carbimazole) are the first-line treatment. In medication-resistant Graves disease, patients can go onto radioactive iodine or thyroidectomy <sup>14,15</sup>.</p><h5>Complications</h5><ul><li>increased risk of <a href="/articles/thyroid-malignancies">thyroid cancer</a> <sup>14</sup>
- +</li></ul><h4>History and etymology</h4><p>It is named after <strong>Robert James Graves </strong>(1796-1852),<strong> an </strong>Irish surgeon who first described it in 1835 <sup>9</sup>, and Carl Adolph von Basedow (1799-1854), a German physician who described it in 1840 <sup>10,11,13</sup>. The Merseburger triad was first described by Basedow, who practised in Merseburg <sup>12,13</sup>.</p><h4>Differential diagnosis</h4><p>For <a href="/articles/hyperthyroidism">hyperthyroidism</a> consider: </p><ul>
- +<li><a href="/articles/marine-lenhart-syndrome-3">Marine-Lenhart syndrome</a></li>
- +<li>toxic <a href="/articles/thyroid-adenoma">thyroid adenoma</a>
- +</li>
- +<li>toxic <a href="/articles/multinodular-goitre">multinodular goitre</a>
- +</li>
- +<li>
- +<a href="/articles/thyroid-inflammatory-conditions">inflammatory</a><ul>
- +<li><a href="/articles/de-quervain-thyroiditis">subacute thyroiditis</a></li>
- +<li><a href="/articles/postpartum-thyroiditis-2">postpartum thyroiditis </a></li>
- +<li><a href="/articles/subacute-lymphocytic-thyroiditis">silent thyroiditis</a></li>
- +</ul>
- +</li>
- +<li>
- +<a href="/articles/pituitary-adenomapitnet">pituitary adenoma</a> </li>
- +<li>extrathyroid origin</li>
- +<li><a href="/articles/struma-ovarii-tumour">struma ovarii</a></li>
- +<li><a href="/articles/metastatic-thyroid-carcinoma">metastatic thyroid carcinoma </a></li>
- +<li><a href="/articles/factitious-hyperthyroidism">factitious hyperthyroidism</a></li>
- +</ul><h4>Practical points</h4><ul><li>patients with Graves disease are at higher risk of <a href="/articles/iodinated-contrast-induced-thyrotoxicosis">iodinated contrast media-induced thyrotoxicosis</a>
Image 10 Nuclear medicine (Thyroid uptake scan) ( update )

Image 11 Nuclear medicine (Thyroid uptake scan) ( update )
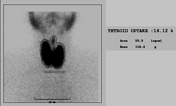
Image 12 Nuclear medicine (Thyroid uptake report) ( create )
