
Multinodular goiter (MNG) is defined as an enlarged thyroid gland (i.e. goiter) due to multiple nodules which may have normal, decreased or increased function.
On this page:
Terminology
When increased activity and hyperthyroidism are present then the condition is referred to as a toxic multinodular goiter or Plummer disease.
Multinodular goiter has been criticized as being a somewhat unhelpful term as some multinodular thyroids are not enlarged, resulting in the unwieldy term "multinodular non-enlarged thyroid" 7.
Clinical presentation
Multinodular goiter is seen in patients in the 35-50 years age range, who present with nodular enlargement in the midline of the neck. It is much more common in females (M:F=1:3). Patients are usually euthyroid, but the nodules may also be hypo- or hyperfunctioning, resulting in systemic symptoms from hypothyroidism or hyperthyroidism, respectively.
Pathology
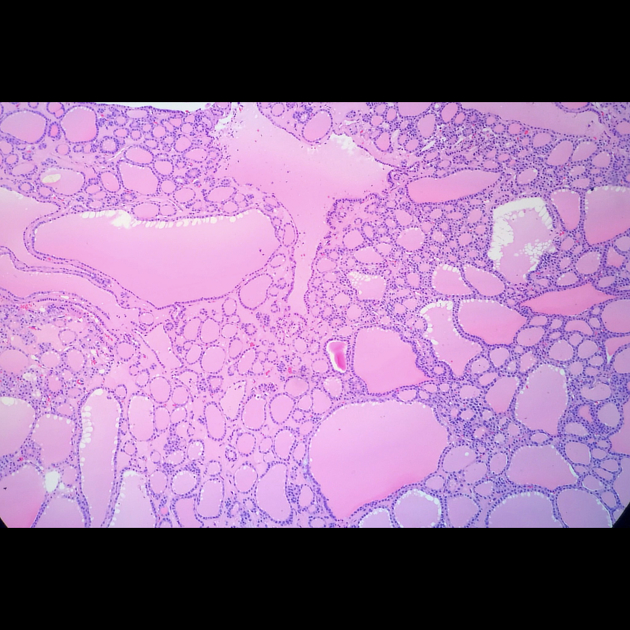
Multinodular goiters develop from simple goiters as a result of repeated instances of stimulation and involution 4.
Most of the nodules are hyperplastic or adenomatous with varying degree of cystic/liquefactive degeneration. Presence of serous/colloid fluid may be noted.
A nodule in multinodular goiter may harbor malignancy. A family history of malignancy and prior neck radiation exposure are known risk factors 2.
Radiographic features
Ultrasound
Sonography remains the first radiological investigation to screen the nodules and look for any suspicion of malignant change in the nodules, which is not uncommon.
Usually, the benign nodules in a multinodular goiter show the following features:
iso- to hyperechoic
surrounding hypoechoic halo
-
spongiform/honeycomb pattern
anechoic areas may contain colloid fluid which may show echogenic foci with comet tail artifacts - see: colloid nodule
peripheral (eggshell) or coarse calcifications
Doppler: peripheral vessels are usually noted; may show intranodular vascularity (mostly in hyperfunctioning nodules)
It is important to screen for the presence of malignant features in any of the nodules and subsequent FNA can be done from the suspicious nodule(s).
Malignant sonographic features
hypoechoic solid
intranodular blood flow
large size: the cut-off is often taken as 10 mm to warrant an FNA
presence of microcalcifications: almost always warrants an FNA
Benign sonographic features
large cystic component
hyperechoic solid
halo
See main article Assessment of thyroid lesions for further details.
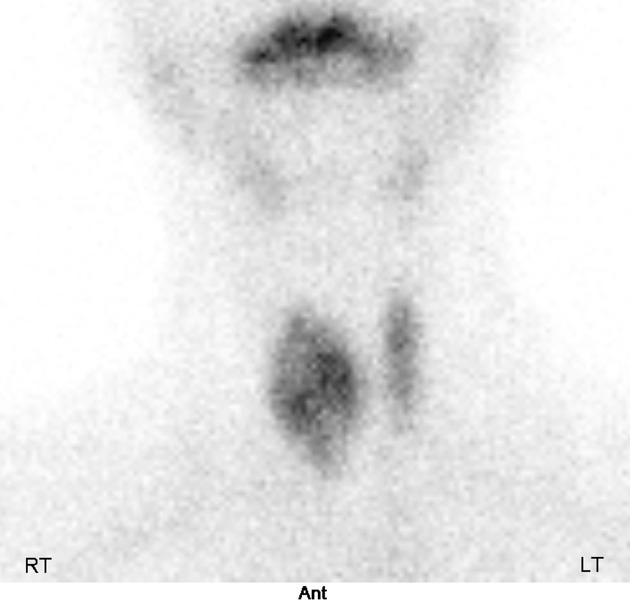
Nuclear medicine
Tc-99m pertechnetate or radioiodine (I-123) demonstrate an enlarged gland, with heterogeneous uptake
-
thyroid uptake scan determines the activity of the gland
a toxic multinodular goiter will show high uptake within the nodules on a background of reduced uptake within the thyroid (cold thyroid)
a non-toxic multinodular goiter will show mild nodular uptake on a background of normal thyroid uptake
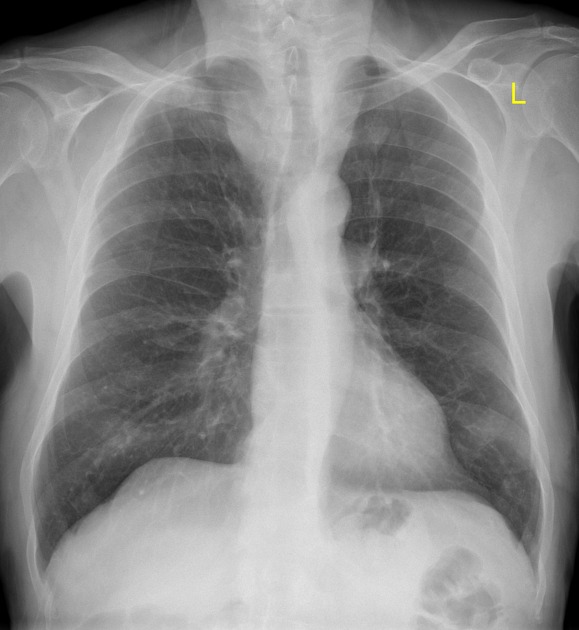
Plain radiograph
goiter is in the differential for an anterior/superior mediastinal mass and is associated with the cervicothoracic sign
associated with deviation of the trachea
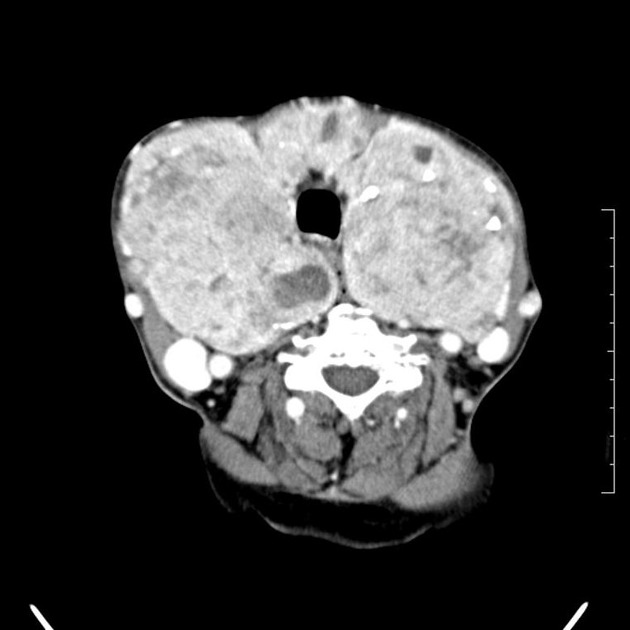
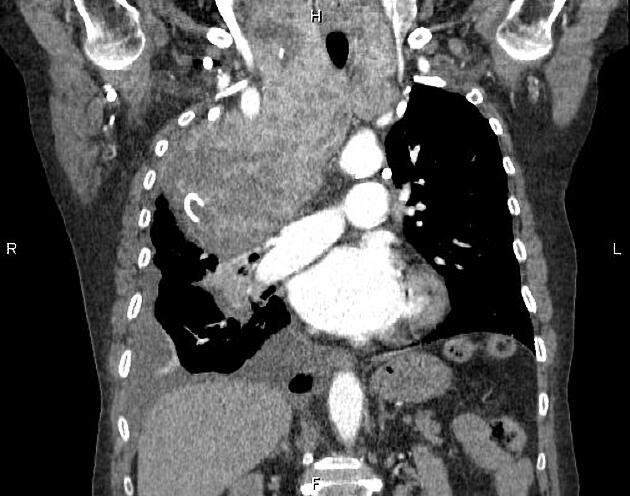
CT
not a primary modality for diagnosis, but goiter may be seen incidentally
CT may be useful for fully characterizing the extent of substernal (retrosternal) goiter
an enlarged and heterogeneous thyroid gland suggests the diagnosis, which is confirmed by ultrasound or scintigraphy
Treatment and prognosis
Treatment of multinodular goiter may be pursued if the thyroid is hyperfunctioning, or if the goiter is causing local mass effect. There is no standard treatment and choice of treatment depends on local practice patterns, the activity of the goiter, and the results of FNA of any suspicious nodules.
surgery: partial or complete resection
-
radioiodine (I-131): occasionally used
dose (in mCi) = (thyroid weight x planned radioiodine delivery to thyroid) / radioiodine uptake
hypothyroidism may occur as an adverse event
Conservative management is also an option as some goiters decrease their rate of growth or may even decrease in size 6.
Practical points
patients with multinodular goiter are at increased risk of iodinated contrast-induced thyrotoxicosis, although this is rare in itself 5,8







 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.