
Hydrocephalus denotes an increase in the volume of CSF, causing the distension of cerebral ventricles (ventriculomegaly) due to insufficient passage of the CSF from its point of production in the ventricles into the systemic circulation, whether that be via resorption into the dural venous sinuses or via the glymphatic pathway 7.
On this page:
Terminology
Although hydrocephalus is typically referred to as either being "obstructive" or "communicating", this can lead to confusion as to the underlying cause of ventriculomegaly as the terms are referring to different aspects of the underlying pathophysiology (namely "why" and "where").
For example, acute subarachnoid hemorrhage confined to the basal cisterns can result in ventriculomegaly by obstructing the normal flow of CSF through the basal cisterns, and by filling the arachnoid granulations. Even though it is mechanistically an obstruction to CSF flow outside of the ventricular system, it is actually considered as a communicating obstructive hydrocephalus.
Since "communicating" hydrocephalus is confusing as it may mean an absorption problem in the arachnoid villi or obstruction of CSF flow to basal cisterns, it is recommended that the terminologies "obstructive" and "non-obstructive" hydrocephalus be used instead to avoid confusion 6.
As such a more precise terminology is to divide hydrocephalus into:
communicating and non-communicating: addressing "where" the obstruction is located
obstructive and non-obstructive: on the grounds of whether or not there is obstruction of CSF pathways in the ventricles or the subarachnoid space 1-3
Pathology
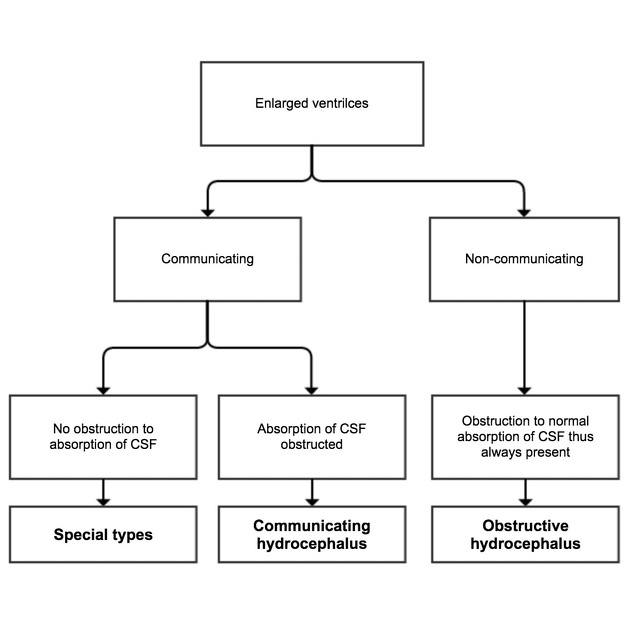
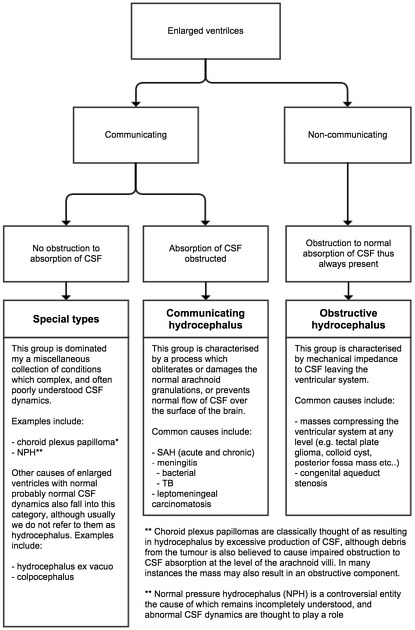
Types of hydrocephalus are as follows (see figures 1 and 2):
-
communicating (i.e. CSF can exit the ventricular system)
-
with obstruction to CSF absorption
usually referred to merely as communicating hydrocephalus
-
passage of CSF from the ventricular system into the subarachnoid space is unimpeded but at some point between the basal cisterns and the arachnoid granulations, normal flow is impeded
subarachnoid hemorrhage (obstruction can be acute when filling the basal cisterns with blood clot, or chronic due to scarring of the subarachnoid space and arachnoid granulations)
-
infective meningitis (both during infection and chronic)
TB meningitis is typically basal filling the basal cisterns
bacterial meningitis is typically also over the convexities
-
without obstruction to CSF absorption
-
a particular group of conditions with disparate, and often poorly understood, abnormal CSF dynamics, including:
choroid plexus papillomas (part of the associated hydrocephalus is thought to be due to overproduction of CSF 1. An obstructive component in larger masses is often also present)
-
additionally, other conditions with large ventricles fall into this group although they are often not thought of as hydrocephalus. These include
hydrocephalus ex vacuo and colpocephaly (ventricles are enlarged due to loss of adjacent brain parenchyma)
-
-
-
non-communicating (i.e. CSF cannot exit the ventricular system, and thus there is by definition obstruction to CSF absorption)
often merely referred to as obstructive hydrocephalus
upstream ventricles are dilated and exert mass effect upon adjacent brain (e.g. effacement of sulci)
-
numerous causes including 8:
fourth ventricle: posterior fossa tumor, or cerebellar infarct or cerebellar hemorrhage
Radiographic features
Frontal horns, bodies, and atria of lateral ventricles are not reliable for hydrocephalus assessment because these areas can easily affected by adjacent cerebral atrophy, resulting in ex vacuo dilatation rather than hydrocephalus 6.
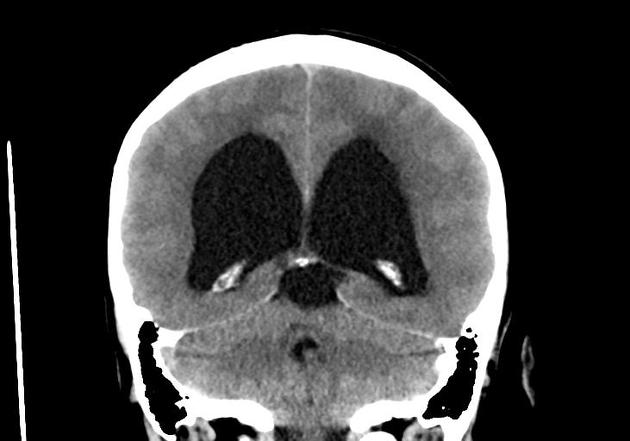
CT
bicaudate index is larger than 95th percentile for age 5
axial width of temporal horn lateral ventricle more than or equal to 5 mm 5
rounding of temporal horn of lateral ventricle
effacement of pericerebral spaces
distension of recesses in third ventricles/bulging third ventricular floor
stretching of corpus callosum. Overstretching can cause detachment of fornix from the splenium of corpus callosum
stretching of septum pellucidum
effacement of basal cisterns in intraventricular obstruction
dilatation of basal cisterns in intracisternal obstruction 6
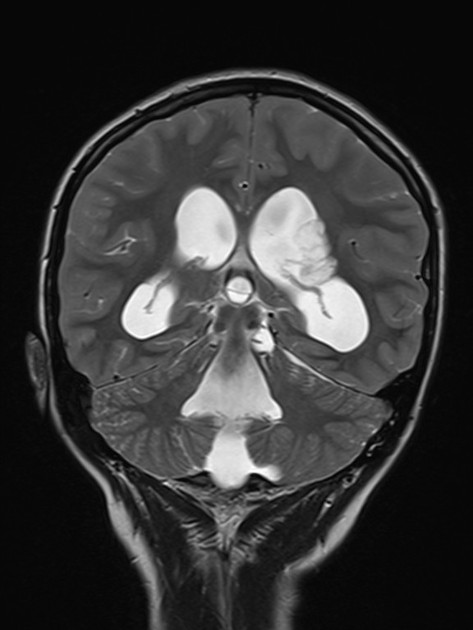
MRI
All the features that can be seen on CT are also seen on MRI with better delineation of the soft tissue structures, tumors, or cysts that cause the obstruction 6.
3D CISS (Siemens)/FIESTA (GE) sequences, based on the balanced steady-state free precession (b-SSFP) sequence, can detect any webs or membrane that causes the obstructions 6.
Diffusion tensor imaging (DTI) sequence can detect degeneration of white matter tracts due to prolonged stretching as a result of the hydrocephalus 6.
History and etymology
Walter Dandy first attempted to classify hydrocephalus into communicating and non-communicating (obstructive) types in 1913 by injecting dyes into experimental animals and later children with hydrocephalus 6. If the dye can be retrieved by lumbar puncture from spinal subarachnoid space, it would mean the hydrocephalus is "communicating". If the dye cannot be retrieved, it would mean the hydrocephalus is "non-communicating" or "obstructive". Although it is widely believed that defective absorption of CSF at the arachnoid granulation is the cause of communicating hydrocephalus; however, obstruction between spinal subarachnoid space and basal cisterns or between the basal cisterns and arachnoid villi are more common. In 1960, Ransohoff recognized this misconception and tried to reclassify hydrocephalus into "intraventricular obstructive" and "extraventricular obstructive". However, his work was largely ignored 6.



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.