
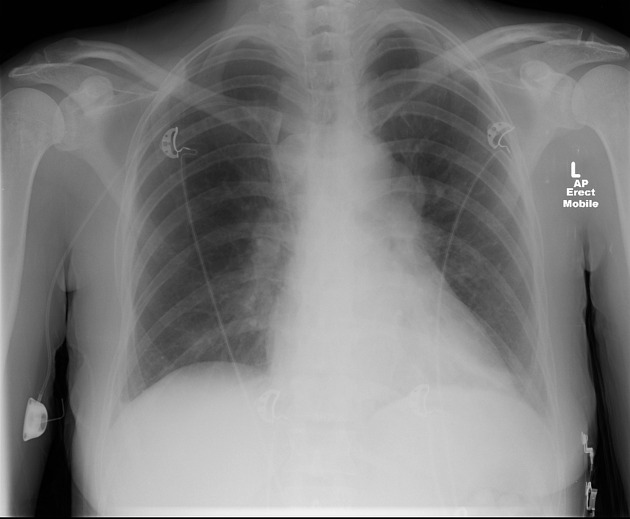
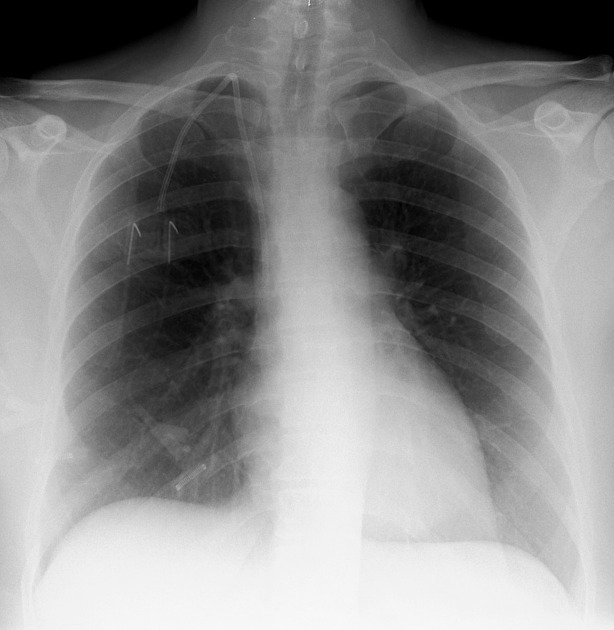
Implantable ports, also known as chemoports, totally implantable central venous access ports or Port-A-Caths, are a type of central venous catheter for patients requiring long-term venous access. They offer long-term central venous access, which is one of the advantages over peripherally inserted central catheters (PICC).
On this page:
Indications
Similar to peripherally inserted central catheters (PICC), implantable ports are primarily inserted to provide long-term central venous access. This is particularly useful for patients who require:
long-term intravenous administration of medication (e.g. chemotherapy or antibiotics)
peripheral access where standard intravenous cannulae insertion is difficult or impossible
to withdraw blood from the body in patients who require frequent blood tests
In comparison to peripherally inserted central catheters (PICC):
implantable ports can last up to several years; PICC lines last for several weeks or months
while PICC lines require daily flushing and dressing, implantable ports require less frequent since they are under the skin
implantable ports are waterproof while a PICC cannot get wet
Contraindications
Absolute
clinically in bacteremia or sepsis with and without neutropenia
Relative
abnormal coagulation profile, prolonged bleeding time
contrast allergy (can be performed without contrast administration)
Procedure
Technique
There are wide variations in technique. The following steps are an example of a technique:
antibiotic prophylaxis is not recommended for routine use 4,5
-
preprocedure ultrasound can be performed to identify an appropriately-sized vein and ensure it is clot free
the most common vein is the right internal jugular vein
other veins include the left internal jugular vein, subclavian veins and inferior vena cava
vessel and port pocket should also not be ipsilateral with the breast cancer site or overlap with the proposed radiation therapy field
-
the vein is punctured under ultrasound guidance, a guidewire is inserted and the proximal end is secured
the distal end of the guidewire is ideally placed in the inferior vena cava
-
the port pocket is created under local anesthesia
the most common site for the pocket is at the pectoral region approximately 2.5 cm from the clavicle
the catheter is inserted using a trocar subcutaneously from the pocket to the vein or vice versa
the peel-away sheath is inserted to facilitate catheter insertion into the venous system
catheter insertion is done during breath hold or inspiration and pinching of the peel-away sheath to minimize air embolism
the catheter tip is adjusted to the superior cavoatrial junction
the distal end of the catheter is attached to the port
the port is anchored to the underlying muscle with sutures
fluoroscopy is used to check for kinks and optimal positioning
aspiration of blood is done to check function
further contrast injection may be performed to reconfirm the tip position and function
the port must be flushed with heparinised saline
the pocket is sutured in two layers and sterile dressings applied
Complications
infection: catheter- or wound-related (most common) 3
tip migration
-
periprocedural
hemorrhage
arrhythmia
arterial puncture: less common with image guidance
-
malposition: less common with image guidance
beware of anatomical variants such as a left SVC
line fracture/embolization
allergic reaction
pinch off syndrome if a subclavian approach is used
infusothorax or chemothorax
History and etymology
The first port implantation performed in an angiography unit using interventional radiology techniques was performed in 1992 2.





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.