
Jugular foramen schwannomas are a rare type of intracranial schwannoma that presents as a jugular fossa mass involving the jugular foramen.
On this page:
Epidemiology
Patients without neurofibromatosis type 2 (NF2) tend to present between the 3rd to 6th decades of life. There is a recognized female predilection 1. The tumors can have a wide variety of clinical presentations.
Pathology
They can arise from cranial nerves IX, X or XI, with IX being the most common 3.
Associations
neurofibromatosis type 2 (NF2): particularly if bilateral
Radiographic features
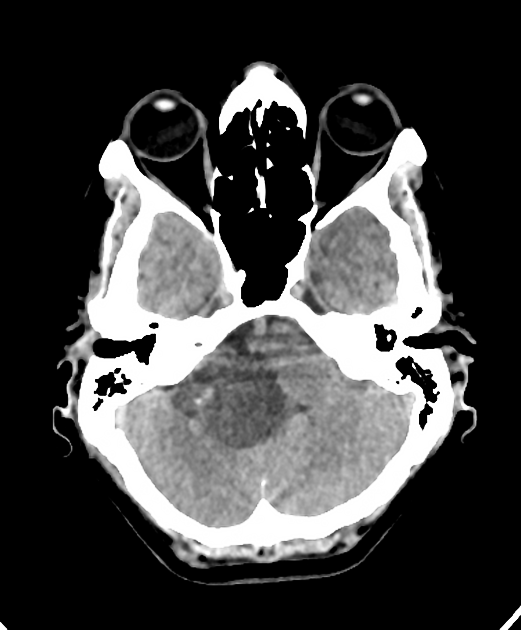
CT
usually well-demarcated
tend to be iso to hypoattenuating to brain parenchyma 3
may show expansion and remodeling of the affected jugular foramen
may have a characteristic dumbbell configuration
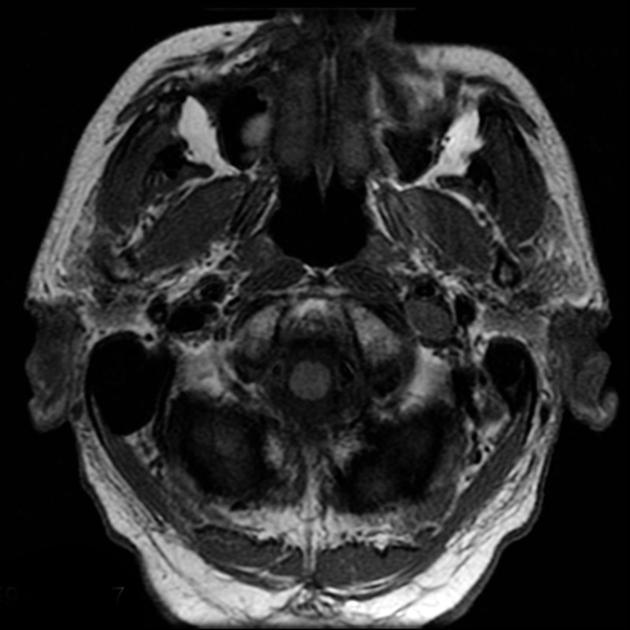
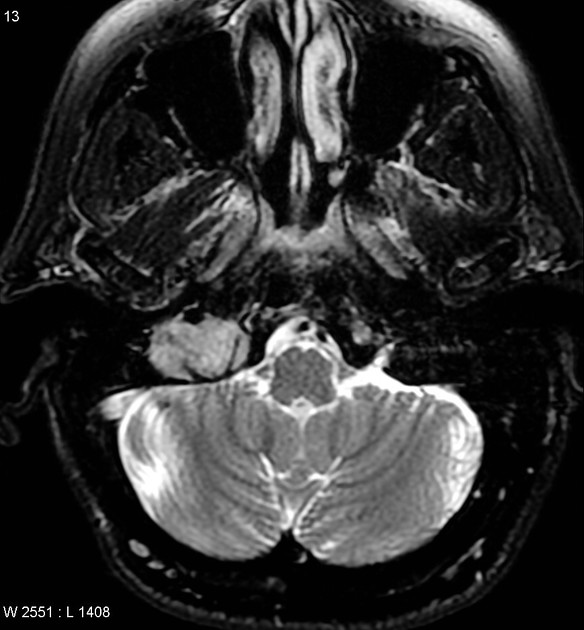
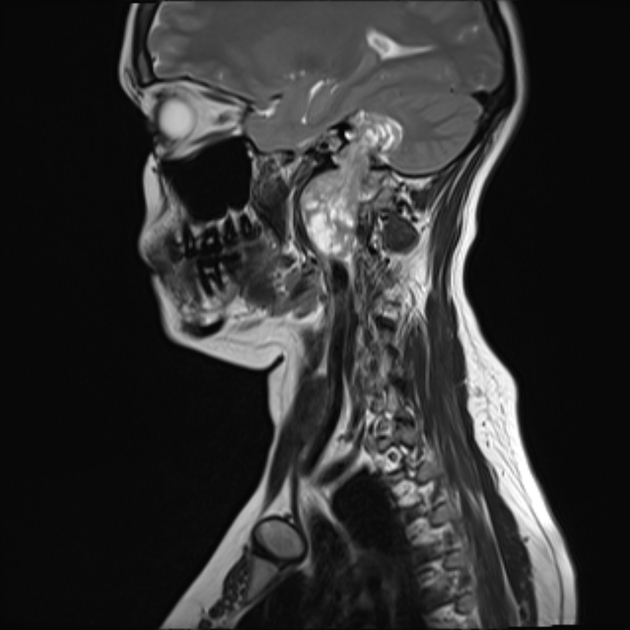
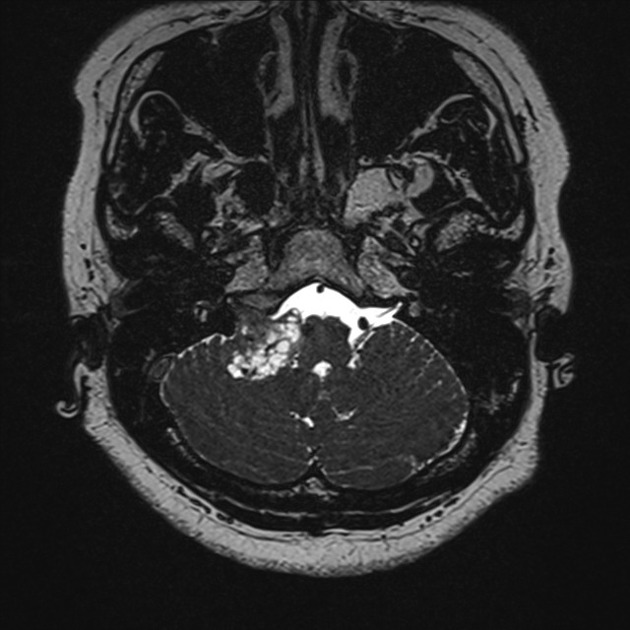
MRI
Signal characteristics are those of a schwannoma:
T1: typically low signal
-
T2: typically high signal
cystic degeneration may be seen in larger tumors
-
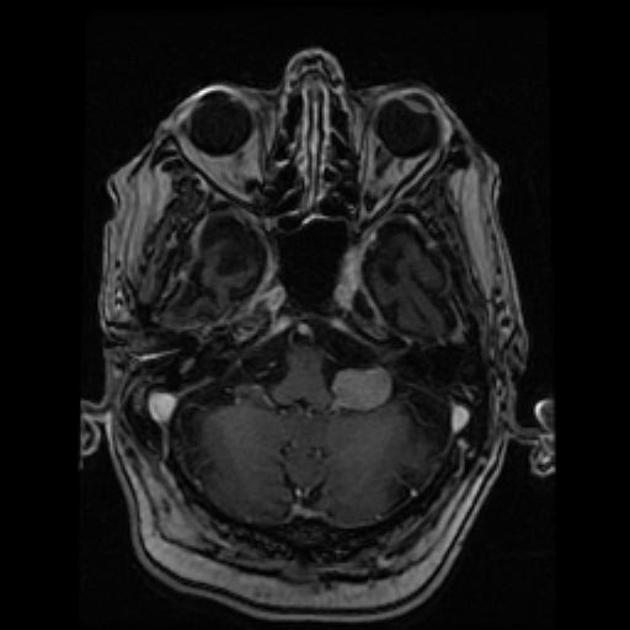
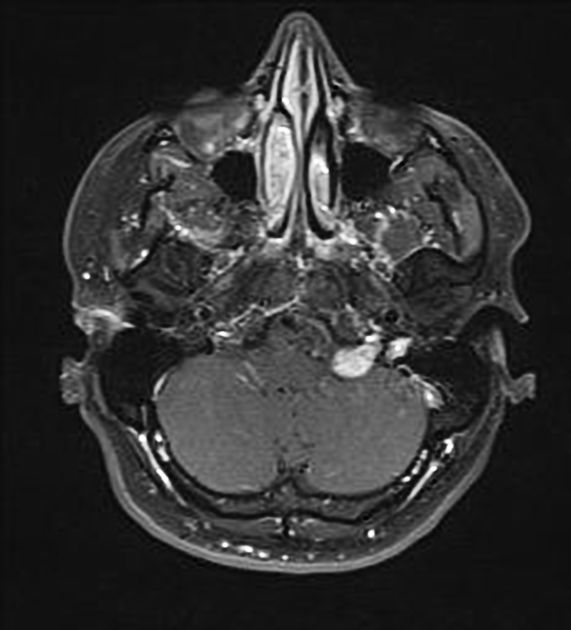
T1 C+ (Gd)
smaller lesions demonstrate intense homogeneous enhancement
larger lesions tend to have heterogeneous enhancement
Treatment and prognosis
As with most schwannomas, they tend to be slow-growing tumors. Surgical resection is often the treatment of choice.
Complications
Differential diagnosis
For a full list of differentials see the article on jugular fossa masses. Considerations in this location include:
-
paraganglioma: jugular paraganglioma
-
“salt and pepper” appearance on MRI with intense contrast enhancement and multiple small flow voids
vascular schwannomas may have peripheral flow voids but should not have internal flow voids
if large, irregular erosion of the margin of the jugular foramen, with decalcification or destruction of the surrounding bone
possible invasion of jugular bulb/vein with intraluminal growth (compared to compression by schwannomas)
-
meningioma around the jugular foramen 2
-
metastatic malignant tumors or lymphoma
may be indistinguishable from schwannoma when involving jugular foramen
most likely destruction of surrounding bone, with less sharply marked borders



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.