
A laryngocele is the dilatation of the saccule of the laryngeal ventricle and is unilateral in the vast majority of cases 8.
On imaging, these lesions are generally characterized as well-defined, thin-walled, fluid or air-filled cystic lesions in the paraglottic space. Communication with the laryngeal ventricle is not always identified, and an extralaryngeal extension through the thyrohyoid membrane may or may not be present.
On this page:
Epidemiology
Almost all laryngoceles are unilateral, and only eight bilateral cases have been reported in the medical literature. The incidence appears to be equally distributed between men and women, and they are most common in mid to later life 8,9.
Risk factors
Raised intralaryngeal pressure secondary to:
excessive cough
playing woodwind/brass instruments
glass blowing
obstructing lesion, e.g. a tumor
childbirth: rarely reported 7
The finding of a laryngocele should prompt a search for an underlying laryngeal carcinoma obstructing the orifice of the laryngeal ventricle 2. Secondary laryngocele is the term used when a tumor is the cause of a laryngocele.
Clinical presentation
When small, the lesions are usually asymptomatic and incidentally discovered when imaging the neck for other reasons. Symptoms vary accordingly to the size and extension of the lesion and may include a sore throat, dysphagia, stridor, neck lump, and/or airway obstruction.
Pathology
Laryngoceles are usually acquired rather than congenital. They are lined by pseudostratified, columnar, ciliated epithelium. Occasional areas of stratified squamous epithelium +/- submucosal serous and mucous glands may be present.
Classification
Three laryngocele subtypes are described 2:
internal (or simple): the dilated ventricular saccule is confined to the paralaryngeal space; it is contained by the thyrohyoid membrane (~40%)
external: the saccule herniates through the thyrohyoid membrane, and the superficial portion is dilated (~25%)
mixed: with dilated internal and external components (~45%)
Radiographic features
Plain radiograph
Laryngoceles are better appreciated on radiographs when they contain air. In these cases, an air pocket may be observed in the upper cervical paralaryngeal soft tissues.
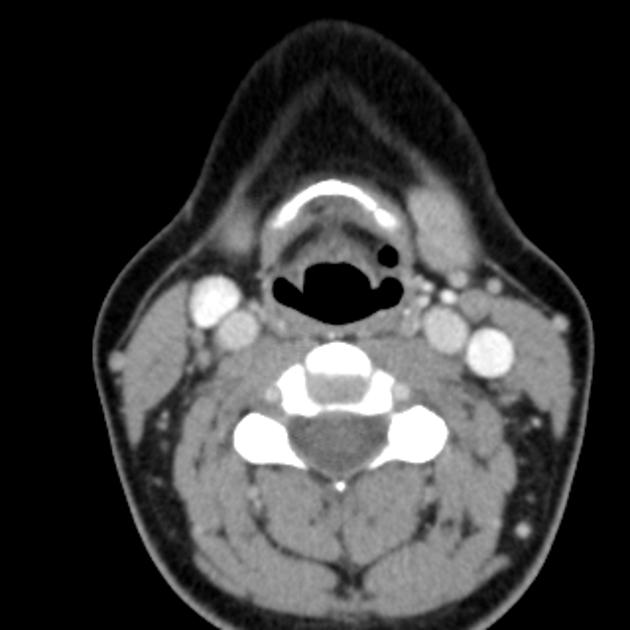
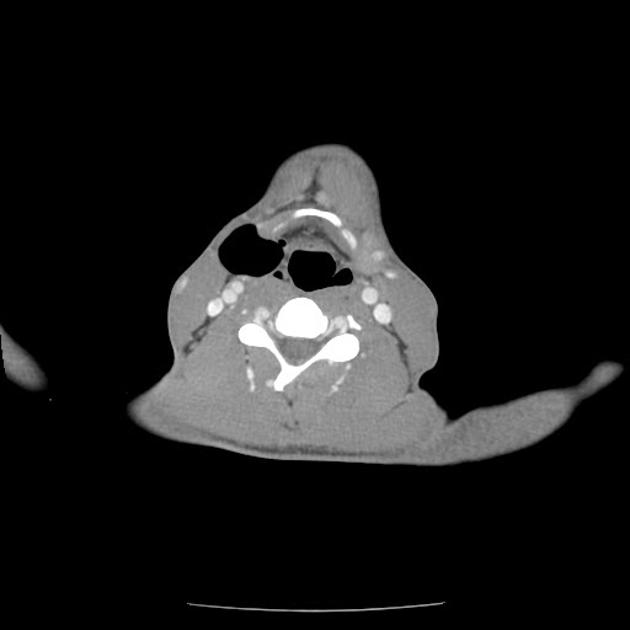
CT
Typically seen as a well-defined, air or fluid-filled lesion related to the paraglottic space which has continuity with the laryngeal ventricle. The extent will depend on the subtype.
Attenuation characteristics may vary depending on laryngocele content, whether air, fluid, and/or mucus.
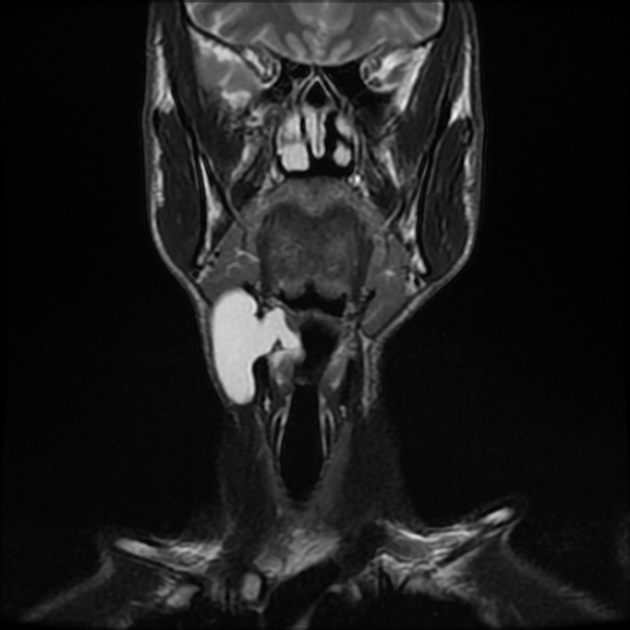
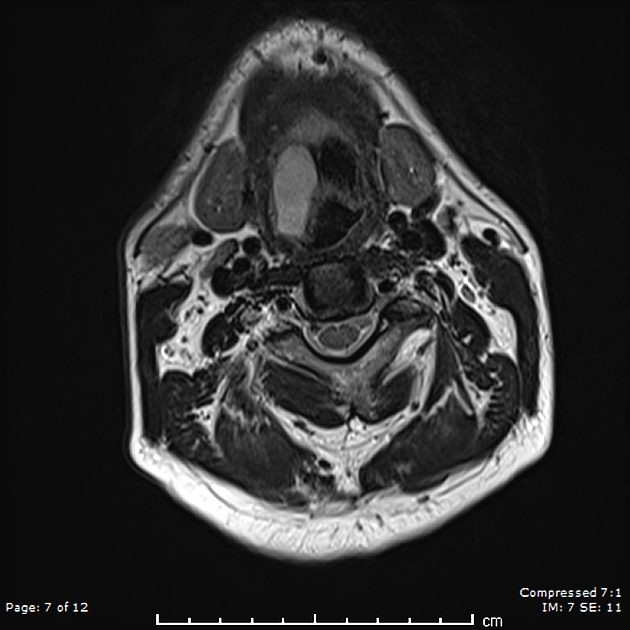
MRI
Demonstrates the same morphological characteristics observed on CT, typically with the following characteristics:
T1: low signal
T2: high signal
T1 C+ (Gd): absent-to-minimal linear peripheral enhancement; when thick enhancing walls are present, consider pyolaryngocele
Treatment and prognosis
Surgical excision may become necessary if a laryngocele is symptomatic 5.
Complications
-
infection: an infected laryngocele is known as a pyolaryngocele
occurs in around 8-10% of laryngoceles 6
infection within a laryngocele can spread to the adjacent head and neck spaces and can lead to supraglottitis
increased risk of laryngeal carcinoma
Differential diagnosis
Imaging differential considerations include:






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.