
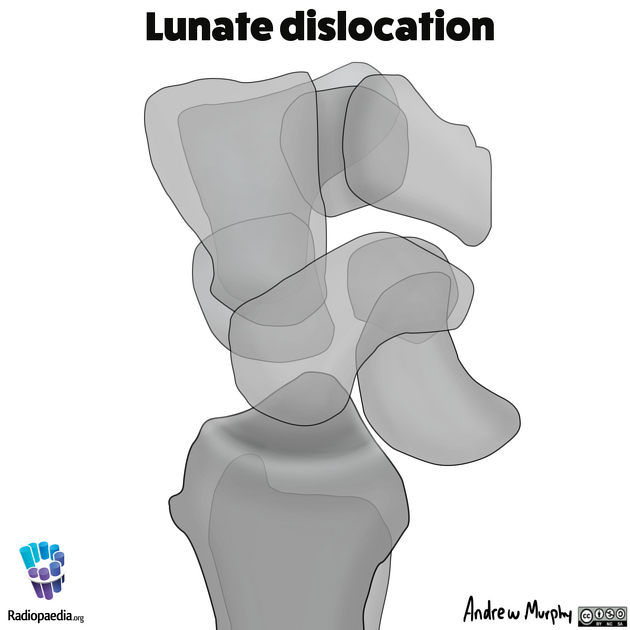
Lunate dislocations are an uncommon traumatic wrist injury that require prompt management and surgical repair. The lunate is displaced and rotated volarly. The rest of the carpal bones are in a normal anatomic position in relation to the radius.
These should not be confused with perilunate dislocations in which the radiolunate articulation is preserved and the rest of the carpus is displaced dorsally.
On this page:
Epidemiology
Lunate dislocations typically occur in young adults with high energy trauma resulting in loading of a dorsiflexed wrist. Overall, carpal dislocations comprise less than 10% of all wrist injuries. Lunate dislocations are far less common than the less severe perilunate dislocation.
Clinical presentation
Patients present with wrist pain following a fall. Volar wrist swelling is usually prominent. The swelling may cause a median nerve palsy due to acute carpal tunnel syndrome. Patients often prefer to hold their fingers in partial flexion due to pain on extension.
Mechanism
Lunate dislocations typically occur due to a fall on an outstretched hand (or during a motor vehicle injury) where there is forceful dorsiflexion of the wrist 3.
There is injury of all of the perilunate ligaments, most significantly the dorsal radiolunate ligament. A four-stage process to describe perilunate instability has been described, where lunate dislocation represents stage IV 2.
Radiographic features
Plain radiograph
-
dislocation is often overlooked
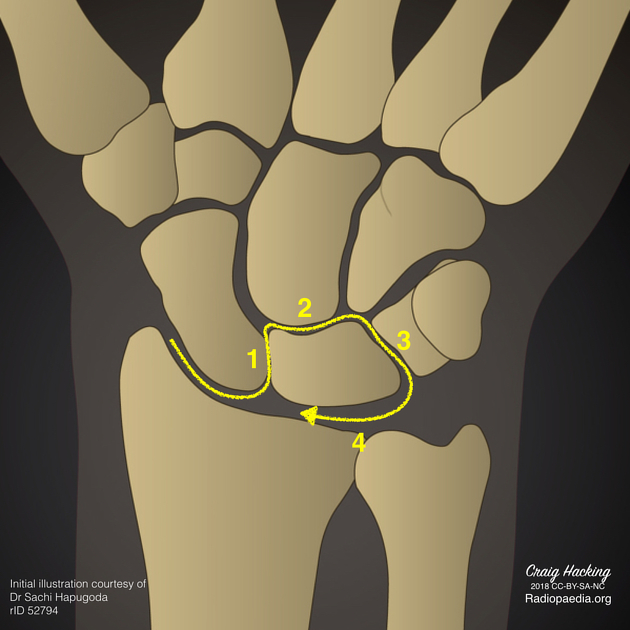
disruption of the normally smooth line made by tracing the proximal articular surfaces of the hamate and capitate
increased radiolunate space
lunate overlaps the capitate and has a "triangular" or "piece of pie" appearance (also seen in perilunate dislocation)
signet ring sign: rounded appearance of the scaphoid tubercle due to rotatory subluxation from injury to the scapholunate ligament
-
lunate seen displaced and angulated volarly
"spilt teacup" appearance
lunate does not articulate with capitate or radius (as opposed to perilunate dislocation where the lunate remains aligned with the radius)
Treatment and prognosis
Urgent reduction and surgical repair of disrupted ligaments is required to prevent long-term joint dysfunction. Despite treatment, there remains a high risk of future degenerative arthritis and wrist instability.
Differential diagnosis
The most important differential is of other carpal dislocations, particularly:
Practical points
In addition to stating that a lunate dislocation is present, a number of features should be sought and commented upon:
-
dislocation
ensure that radiolunate alignment is disrupted, and that you are not looking at a perilunate dislocation (stage II carpal dislocation)
evaluate and comment on the degree or palmar rotation of the lunate (this can be up to 270 degrees) 4
ensure that the capitate remains co-linear with the long axis of the radius
any additional fractures
















 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.