
Möbius syndrome, also known as congenital facial diplegia syndrome, is a rare congenital condition characterized by the absence or underdevelopment of the nuclei of the abducens (CN VI) and facial nerve (CN VII).
On this page:
Epidemiology
Möbius syndrome is rare with an estimated incidence of ~1 case per 100,000 births 4.
Clinical presentation
The earliest sign is the inability of the newborn to suckle, with an expressionless face, and drooling. Paralysis may be unilateral or bilateral.
As individuals grow older, most conspicuous signs are an inability to close their mouths or smile. Inability to blink may lead to corneal abrasions.
Pathology
Etiology is multifactorial, and several theories have been proposed, with the most supported theory being of a transient ischemic or hypoxic insult to the fetus. Infectious and genetic etiologies have also been proposed.
Additional brainstem involvement is also common and may include other cranial nerves as well as the musculoskeletal system. Grading schemes have been proposed which include additional manifestations (e.g. CLUFT (cranial nerve, lower limb, upper limb, face, and thorax)).
Associations
The combination of Möbius syndrome and Poland syndrome has been well described (thus Poland-Möbius syndrome) 3.
Radiographic features
MRI
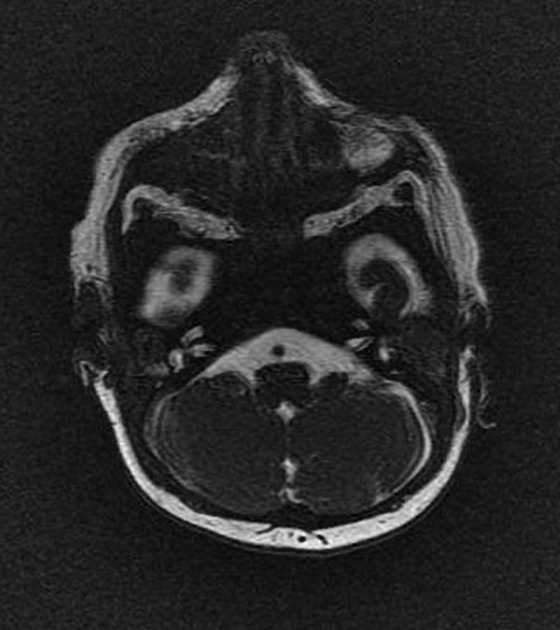
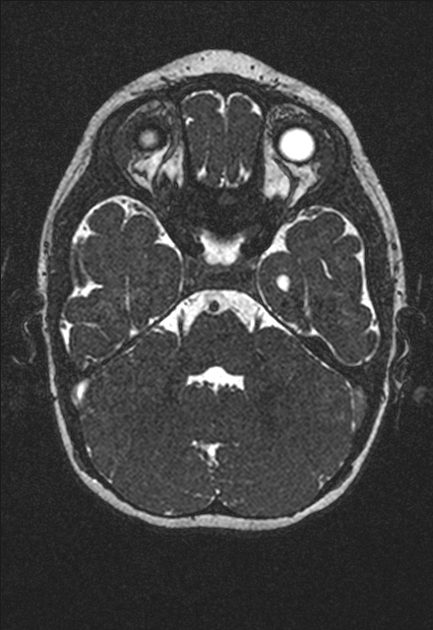
High resolution cisternographic sequences (e.g., CISS, FIESTA) best demonstrate absence or hypoplasia of cranial nerves VI (in the prepontine cistern) and VII (in the cerebellopontine angle cistern and internal auditory canal).
Conventional MRI uniformly demonstrates straightening of the floor of the fourth ventricle as a result of absence of the facial colliculus 5. In addition, in most cases, the pons is hypoplastic (length of the pons less than twice the length of the midbrain) 5.
Other associated findings present in a minority of cases include the following, roughly in decreasing frequency 5:
- midbrain malformation characterized by tectal beaking, fusion of the quadrigeminal inferior colliculi, increased anteroposterior diameter of the mesencephalon, and shallow interpeduncular cistern
- thalamic fusion
- periventricular nodular heterotopia
- arachnoid cysts in the middle or posterior cranial fossae
- ventriculomegaly without obstructive hydrocephalus, especially frontal horn prominence
- corpus callosum dysplasia
- hippocampal malrotation
- cerebellar hypoplasia, especially vermian hypoplasia
- cerebral aqueduct stenosis with hydrocephalus
Treatment and prognosis
The disease is not progressive.
Various plastic surgery procedures can be performed to attempt to recover facial muscles function. For example, microvascular transfer of a gracilis muscle to the face.
History and etymology
The clinical syndrome was first described by Paul Julius Möbius (1853-1907): German neurologist.
Differential diagnosis
Other congenital disorders have overlapping imaging appearances 5:


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.