
Musculoskeletal angiosarcomas, (along with hemangiopericytomas and hemangioendotheliomas) are tumors that arise from vascular structures. They are typically difficult to distinguish from one another on imaging alone.
Angiosarcomas, are the most aggressive of the three, frequently having metastases at the time of diagnosis, and often having local recurrences.
On this page:
Epidemiology
They are more frequently seen in males (M:F 2:1) except when seen in the setting of post-mastectomy lymphedema which is clearly more common in women and is known as the Stewart-Treves syndrome.
Pathology
Location
They can occur in:
skin: 33%
soft tissues: 24%
-
-
long bones: 60%
tibia: 23%
femur: 18%
humerus: 13%
pelvis: 7%
-
Histology
Histologically they can contain either hemangiomatous or lymphangiomatous cellular elements, which accounts for them previously being referred to as lymphangiosarcomas or haemangiosarcomas.
Radiographic features
Radiologically they appear quite similar to hemangiopericytomas and hemangioendotheliomas.
Plain radiograph
May be seen as a non-specific soft tissue mass. When involving bone, they are predominantly lytic, and may mimic hemangiomas with a course honeycomb appearance.
Angiography (DSA)
Dense, well-circumscribed areas of enhancement with early draining veins and shunting. Hemangiopericytomas are described as having a pedicle formed by the arteries supplying the tumor from which vessels branch to encircle the tumor.
CT
Non-specific soft tissue mass, with a density similar to muscle but demonstrating bright contrast enhancement. CTA may demonstrate large feeding vessels.
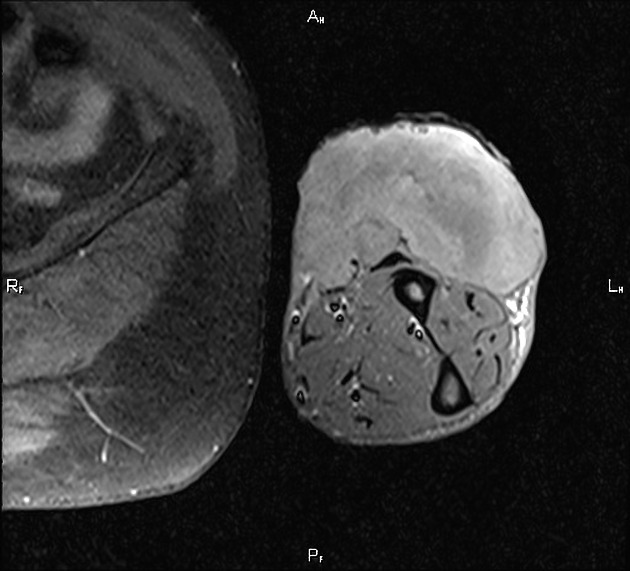
MRI
Brightly enhancing soft tissue mass, often hyperintense on T2WI, with prominent flow voids, most marked in hemangiopericytomas.
See also
angiosarcoma (general article)


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}