
Oculomotor nerve palsies, or third nerve palsies, result in weakness of the muscles supplied by the oculomotor nerve, namely the superior rectus, inferior rectus, medial rectus, inferior oblique, and levator palpebrae superioris muscles.
On this page:
Terminology
If the pupil is normal-sized and reactive to light, it is called a pupil-sparing third nerve palsy; conversely if the pupil is enlarged and non-reactive, it is called a non-pupil sparing third nerve palsy.
Clinical presentation
Classically, patients present with diplopia and physical exam findings ipsilateral to the oculomotor nerve (CN III) lesion:
-
"down and out" ocular positioning
abduction, slight depression, and intorsion (due to paralysis of adduction, elevation, and depression)
-
complete ptosis
due to neuropathy affecting levator palpebrae superioris
-
+/- enlarged unreactive pupil
if present, suggests compression of CN III, because the parasympathetic pupillary fibres are located peripherally in the nerve and are more likely affected by external compression
Pathology
Aetiology
It has numerous possible aetiologies which can be divided according to which portion of the nerve is affected:
dorsal midbrain (nuclear lesions): usually due to small regions of infarction; often no other neurological symptoms
ventral midbrain (fascicular): Benedikt syndrome and Weber syndrome
-
interpeduncular (subarachnoid)
-
posterior communicating artery aneurysm
rapidly enlarging with or without SAH is the most common cause, and usually involves only the oculomotor nerve
ischaemic involvement of the nerve will usually be pupil sparing whereas aneurysmal compression usually involves the pupil
basal meningeal processes including infection, neoplastic infiltration, and inflammatory lesions (e.g. sarcoidosis) often involve additional cranial nerves
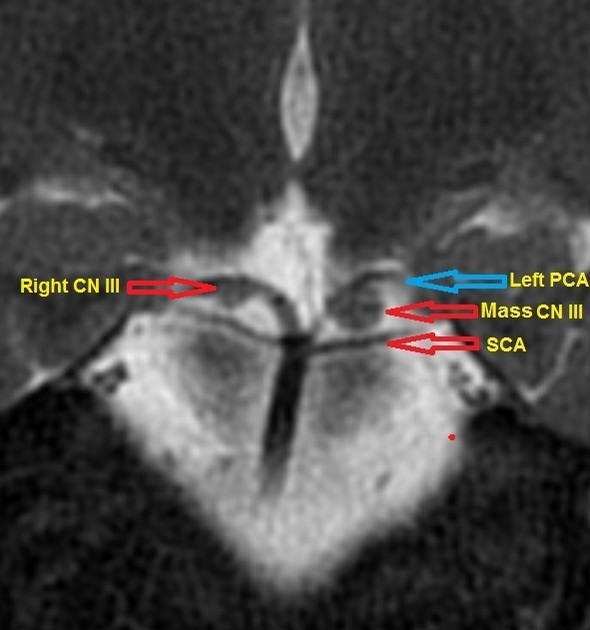
neurovascular compression without aneurysm 3
-
-
cavernous sinus portion
neoplasms, most commonly pituitary macroadenomas extending into the sinus, meningiomas of the sella or sinus and any other sinus mass (e.g. trigeminal schwannomas) can compress the nerve against the interclinoid ligaments
when the process is more diffuse, such as in cavernous sinus syndrome, other cranial nerves are also involved (e.g. Tolosa-Hunt syndrome)
-
orbital portion
usually there is associated proptosis or other focal orbital signs
conditions include intraorbital tumours (optic nerve glioma, optic nerve meningioma) and inflammatory orbital pseudotumour
Treatment and prognosis
In post-traumatic oculomotor nerve palsy, gaze movement training and steroid injections may be helpful 2.



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.