
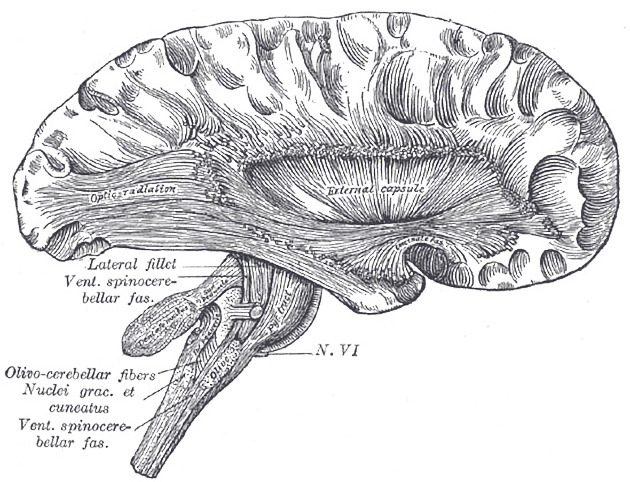
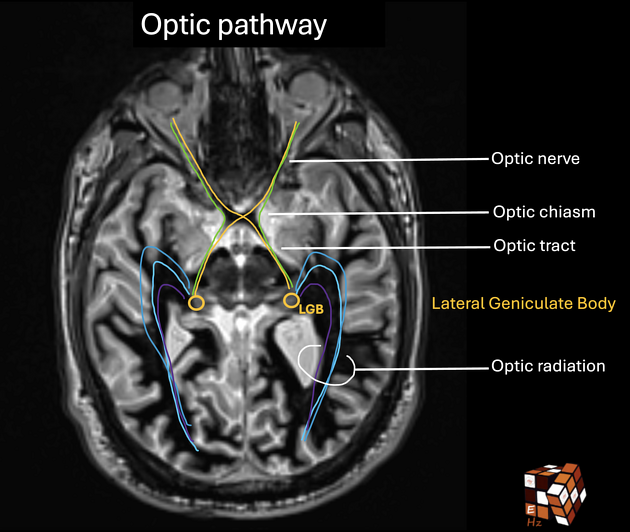
The optic radiation, also known as geniculocalcarine tract, is part of the visual pathway, forming the connection between the lateral geniculate nucleus of the pulvinar of the thalamus with the primary visual cortex of the occipital lobe.
This pathway is formed by the axons of neurons correlating to the contralateral visual field. For example, the left-sided radiations contain information from the left temporal and right nasal retina. Temporal fibers synapse at layers 2, 3 and 5 of the lateral geniculate nucleus, while nasal fibers at layers 1, 4, and 6. The inferior fibers of the optic radiation correlate with the superior visual field. M-type retinal ganglion cells synapse in layers 1 and 2, while P-type in 3-6.
On this page:
Images:
Gross anatomy
Anatomically, the optic radiations resemble a flattened sheet of white matter. From their origin at the lateral geniculate nucleus, the optic radiations pass through the retrolentiform part of the internal capsule as the posterior thalamic radiation and spread out into three main bundles:
anterior bundle (Meyer loop)
central bundle
posterior bundle
Anterior bundle (Meyer loop)
The anterior bundle (Meyer loop) travels anterolaterally along the roof of the temporal horn of the lateral ventricle prior to taking a sharp turn anteroinferiorly around the temporal horn of the lateral ventricle. At this point, its anterior border is ~4.5mm anterior to the temporal horn and is intermingled with anterior commissure fibers. The anterior bundle then tracks backwards, deep to the superior and middle gyri of the temporal lobe, remaining lateral to the temporal horn of the lateral ventricle. The anterior bundle synapses in the anteroinferior border of the calcarine sulcus.
Central bundle
A central bundle of fibers initially traverses laterally over the roof of the temporal horn of the lateral ventricle, prior to sharply turning posteriorly and continuing laterally along with the occipital horn of the lateral ventricle. The tapetum separates it from the wall of the posterior horn. This bundle travels superiorly to the anterior bundle until synapsing in the posterior calcarine sulcus. The central bundle travels deep to the superior gyrus of the temporal lobe and is related to the auditory radiation (sublentiform internal capsule) and inferior longitudinal fasciculus.
Posterior bundle
The posterior bundle tracks dorsally and posteriorly, separated from the lateral wall and roof of the occipital horn of the lateral ventricle only by the tapetum. This posterior bundle is relatively superior to both anterior and central bundles and terminates in the superior lip of the calcarine sulcus.
In their relation to the posterior horn of the lateral ventricle, the tapetum and optic radiation together make up the sagittal stratum, which runs in a craniocaudal direction.
Relations
Key relations of the optic radiations include;
retrolentiform internal capsule (all bundles)
anterior temporal horn of lateral ventricle (Meyer’s loop)
proximate to the roof and lateral wall of the lateral ventricle (Meyer’s loop and central bundle)
lateral wall and roof of the posterior horn of lateral ventricle; separated by the tapetum (Meyer’s Loop – inferior, central bundle – middle, posterior bundle – superior including roof)
Related pathology
Optic radiation damage
anterior +/- central bundle; homonymous superior quadrantanopia ("pie-in-the-sky" deficit)
posterior +/- central bundle; inferior or "pie-in-the-floor" deficit
macular vision may be spared in these lesions, particularly if the lesion is in the occipital lobe
Vascular lesions
-
lesions affecting the anterior or lateral choroidal arteries may affect the lateral geniculate nucleus
the lateral aspect corresponds to the superior visual field
the medial aspect corresponds to the inferior visual field
anterior choroidal artery supplies both medial and lateral parts of the lateral geniculate nucleus; an occlusion lesion results in a (usually incomplete) peripheral wedge-shaped homonymous hemianopia
lateral choroidal artery supplies the hilum of the lateral geniculate nucleus; an occlusion here may cause a homonymous horizontal quadrantanopia (i.e. lateral “pie defect”)
middle cerebral artery and posterior cerebral artery infarcts may affect the radiations distal to the lateral geniculate nucleus, and can cause a range of clinical presentations from small homonymous quadrantanopias to dense homonymous hemianopias; these changes are often part of a larger stroke syndrome
ischemic and hemorrhagic changes in perforating arteries branching from the MCA and PCA (lateral lenticulostriate, thalamogeniculate), as well as anterior choroidal artery territories, may cause field defects
occipital cortex lesions tend to cause homonymous hemianopias of variable size – with or without macular involvement; the MCA may supply the distal tip of the occipital lobe, corresponding to the macula
Neoplastic lesions
temporal and parietal lobe invasive tumors (i.e. glioma, metastasis) can cause visual field losses relative to their location and may be discovered during investigation for visual field defects
lesions in the parietal lobe are associated with paresthesia, inattention, neglect, apraxia, agnosia, and speech difficulties
temporal lobe lesions are associated with memory, auditory, speech and vestibular disturbances, as well as seizures.
it is rare for mass effect lesions to present with isolated optic radiation type field deficit
Inflammatory/degenerative conditions
Multiple sclerosis, periventricular leukomalacia, adrenoleukodystrophy (children) may produce mixed, or non-specific field defects.
Iatrogenic
Given the course of the optic radiation through the anterior temporal lobe, and relation to the inferior basal nuclei, Meyer’s loop may be damaged in anterior temporal lobectomies (50-90%) and amygdalohippocampectomies (50%).



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.