
Peripheral nerve sheath tumours (PNSTs) are a group of primary neurogenic tumours that arise from nerve sheaths outside of the central nervous system. The vast majority are benign, however, malignant transformation is seen particularly in large tumours and those associated with neurofibromatosis type 1 (NF1).
On this page:
Clinical presentation
Symptoms of benign peripheral nerve sheath tumours are non-specific and include sensory and/or motor deficits, isolated pain, painful mass (i.e. positive Tinel sign), asymptomatic mass or may be incidental 12.
Pathology
Markers
Many peripheral nerve sheath tumours express somatostatin receptors 6.
Classification
Their imaging appearances, demographics, treatment, and prognosis vary greatly, and these are discussed separately.
The WHO classification of tumours of soft tissues recognises a variety of peripheral nerve sheath tumours:
-
benign
-
malignant
Radiographic features
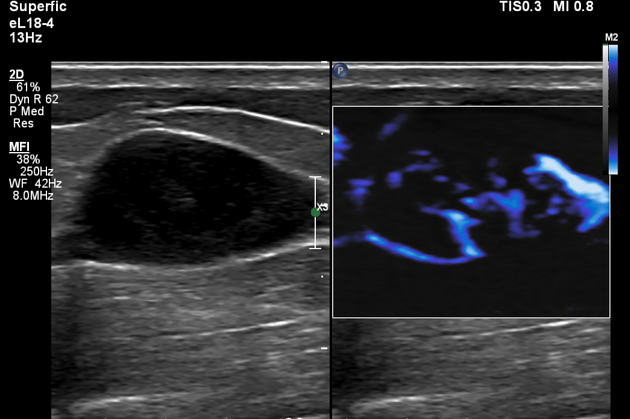
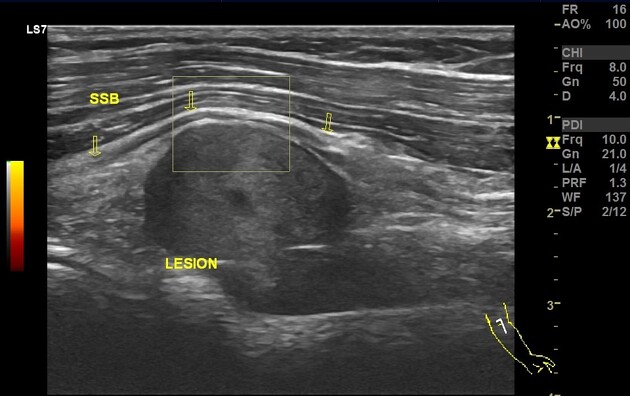
Ultrasound or MRI, the latter considered gold-standard, may suggest a neurogenic origin of a soft tissue mass and whether there are benign or malignant features, however, in most cases, imaging cannot reliably distinguish between the different histological subtypes 9.
Usually, a presumptive diagnosis is made taking into account patient demographics, pre-existing conditions (e.g. neurofibromatosis type 1 or type 2), the location and size of the tumour, and evidence of rapid growth.
Shared imaging features are discussed below.
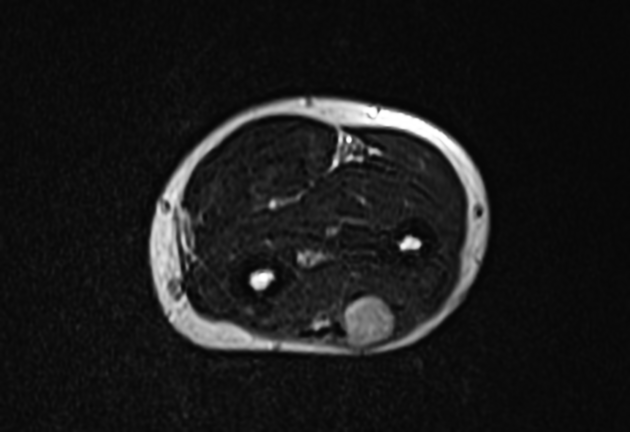
MRI
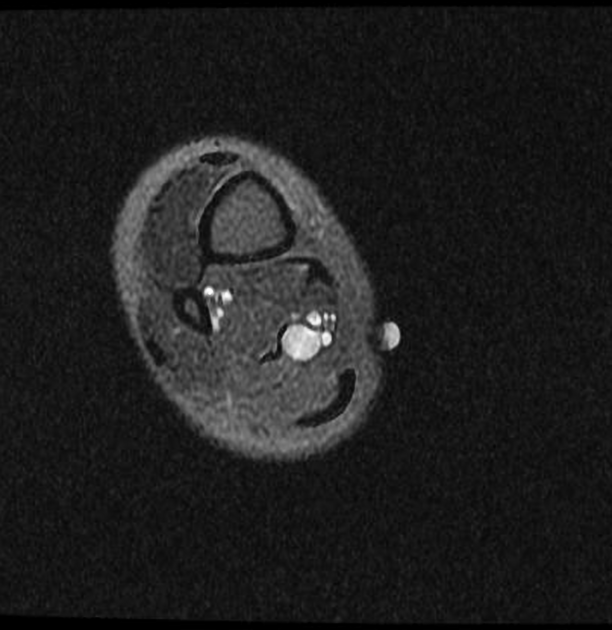
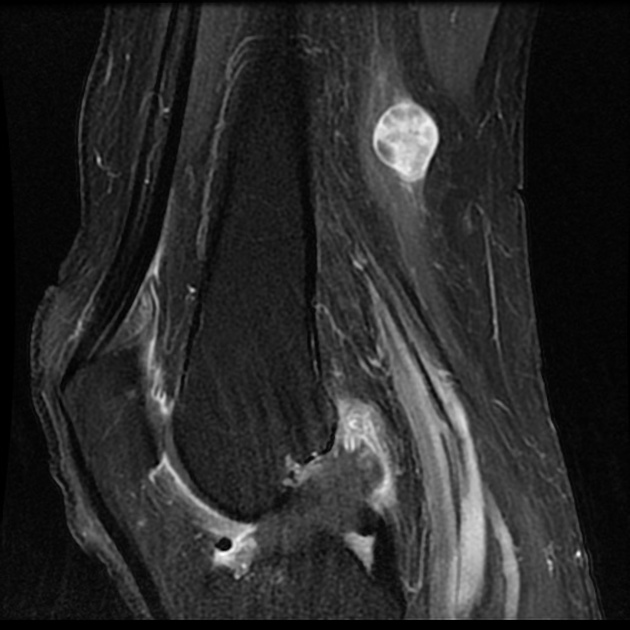
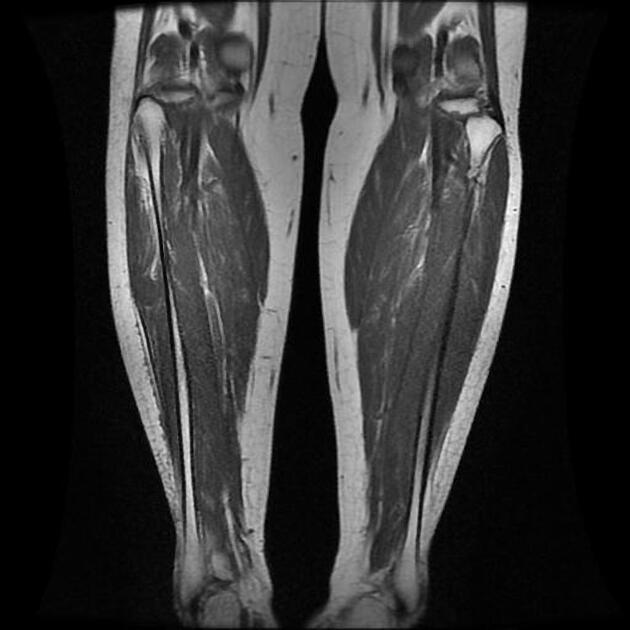
As a group, localised peripheral nerve sheath tumours demonstrate the following features:
fusiform or round mass 9 with tapered ends
tail sign: direct continuation a nerve into and/or out of the mass 9
denervation changes in muscles supplied by the involved nerve 9
Treatment and prognosis
Surgical resection is the treatment of choice, not only for diagnostic confirmation (i.e. histopathology) and also with curative intent 9.
Pre-surgical biopsy of peripheral nerve sheath tumours (usually an ultrasound-guided core biopsy) is typically reserved for lesions with indeterminate or malignant clinical and/or radiological features; the risk of biopsy (e.g. new/worsening neuropathic pain or sensory/motor impairment) outweighs the benefit of biopsy in suspected benign peripheral nerve sheath tumours 10,11.
Differential diagnosis
Considerations include 7,8:
benign and malignant myxoid tumours, e.g. myxoid liposarcoma, myxofibrosarcoma, fibromyxoid sarcoma






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.