
Posterior cerebral artery (PCA) infarcts arise, as the name says, from occlusion of the posterior cerebral artery. It is a type of posterior circulation infarction.
On this page:
Epidemiology
Posterior cerebral artery strokes are believed to comprise approximately 5-10% of ischaemic strokes 6.
Clinical presentation
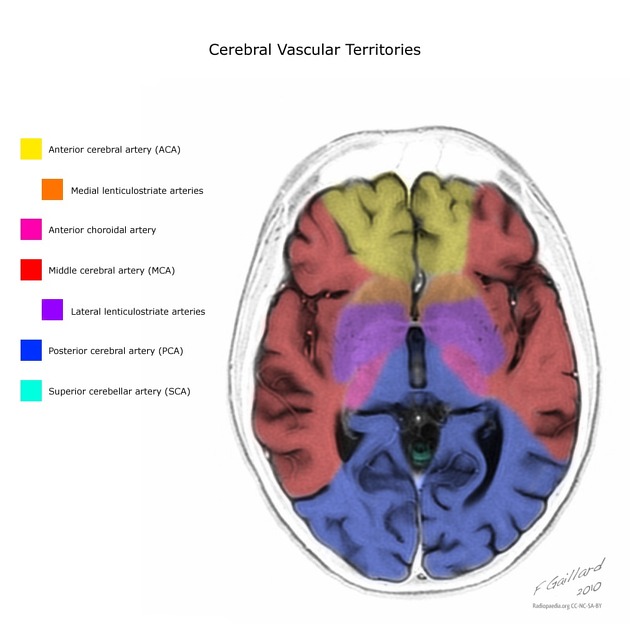
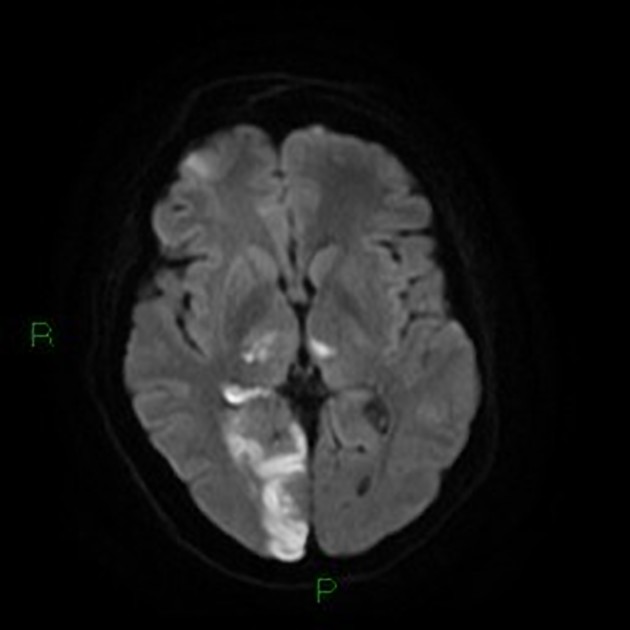
Symptoms of posterior cerebral artery stroke include contralateral homonymous hemianopia (due to occipital infarction), hemisensory loss (due to thalamic infarction) and hemi-body pain (usually burning in nature and due to thalamic infarction) 3. If bilateral, often there is reduced visual-motor coordination 3. It is generally considered that sensory loss and hemianopia unilaterally without paralysis, is diagnostic of PCA territory stroke 4.
Because the PCA supplies the thalamus, PCA infarction can lead to contralateral thalamic syndrome.
Pathology
The most common causes of PCA strokes include atherosclerosis, small artery disease and embolism 5.
Treatment and prognosis
Depending on the timing (within 4.5 hours), patients may be eligible for thrombolysis (c. 2012) 4. If they present after this window, patients may be suitable candidates for endovascular treatments (including stenting, angioplasty, mechanical embolectomy, etc.), however, evidence for mechanical thrombectomy in PCA strokes has not yet been fully established (c. 2021) as all major thrombectomy trials did not include strokes involving the posterior circulation 5, 6.
The size of the vessel and unclear symptoms onset can make the treatment of acute ischaemic stroke challenging 5.












 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.