
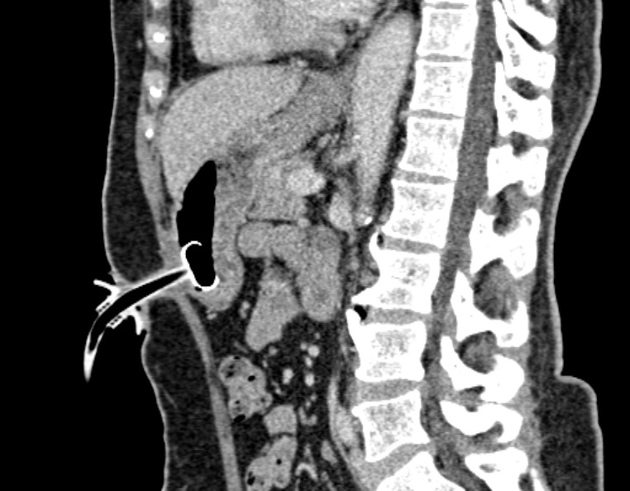
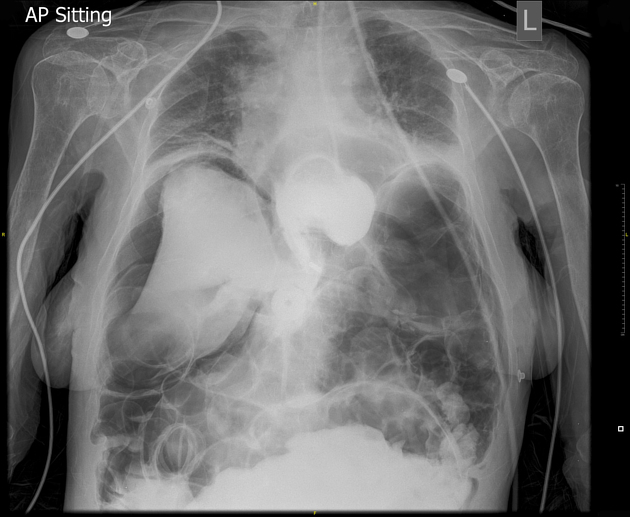
A radiologically inserted gastrostomy (RIG), or percutaneous radiological gastrostomy (RPG), is a procedure where a gastrostomy tube is inserted percutaneously into the stomach under fluoroscopic guidance, principally to provide nutritional support for patients with swallowing disorders 1. Gastrostomy tubes otherwise can be inserted endoscopically, known as a percutaneous endoscopic gastrostomy (PEG).
Indications
inadequate oral intake due to dysphagia (neurologic disorder, oesophageal obstruction, head & neck masses)
decompression of gastric contents
Contraindications
Absolute contraindications
Some generally accepted absolute contraindications are 2:
severe coagulopathy
dangerous percutaneous access to the stomach (e.g. interposed colon)
Relative contraindications
infection or neoplasia along the percutaneous tract
prior gastric surgery
severe gastro-oesophageal reflux
Procedure details
Prior to the procedure, review prior imaging studies to choose the best percutaneous approach. The patient should be fasted for 8 hours 2.
place a nasogastric tube
administer conscious sedation
insufflate air via the nasogastric tube to distend the stomach. Enough air should be used to distend the stomach and oppose the gastric wall to the anterior abdominal wall (~250-500 mL).
choose a puncture site in the body of the stomach, equidistant from the lesser and greater curvatures
infiltrate local anaesthesia with about 10 mL of 1% lidocaine along the percutaneous tract
make a small skin incision with a #11 scalpel
use a gastropexy device (e.g. a 17G needle preloaded with a Cope suture anchor) to puncture the stomach. One should feel and see the anterior stomach wall tenting upon pressure, then a give a sharp jab to enter the gastric lumen
confirm correct location by aspirating air into the syringe
advance a stylet in the gastropexy device, to discharge the anchor in the stomach
the stylet and gastropexy needle are then removed and the stomach is approximated to the anterior abdominal wall by gentle traction on the anchor
make another gastric puncture which will be used for the gastrostomy tube. For a simple gastrostomy, one should aim vertically down or slightly towards the fundus. However, if conversion to a gastrojejunostomy is anticipated, the needle should be directed towards the pylorus
confirm intraluminal localisation with a small amount of contrast medium, which will outline gastric folds
insert a 0.038-inch J-tipped stiff guidewire and loop it in the stomach before withdrawing the needle
introduce serial fascial dilators over the guidewire to dilate the muscular layers of the stomach, while taking care to keep tension on the anchor and to keep the guidewire inside the stomach lumen
insert the selected gastrostomy tube over the wire using a peel-away sheath
inflate the gastrostomy balloon with the required amount of sterile water (e.g. 5-10 mL)
confirm proper position of the tube, then apply gentle tension on the gastric wall by pulling the tube while applying the retention disc on the skin, which will fix the anterior gastric wall to the anterior abdominal wall
fix the retention disc on the skin with a non-absorbable suture
Some interventional radiologists perform RIG without gastropexy, using a single puncture.
Complications
Potential complications include 2,3:
haemorrhage
wound infection
gastrointestinal perforation
migration





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.