
Susac syndrome, also known as retinocochleocerebral vasculopathy or SICRET syndrome (small infarctions of cochlear, retinal and encephalic tissue), is a rare syndrome typically affecting young to middle-aged women that is clinically characterized by the triad of acute or subacute encephalopathy, bilateral sensorineural hearing loss, and branch retinal arterial occlusions.
On this page:
Epidemiology
The condition more commonly affects females around the 2nd to 4th decades 1. Approximately three females are affected for every male case 1.
Diagnosis
Diagnostic criteria have been proposed in 2016 that divide patients into definite and probable diagnosis of Susac syndrome based on the presence of certain clinical and imaging criteria 18. These require cerebral MRI with contrast, fluorescein angiography and audiometry.
The criteria are:
-
brain involvement
-
i. symptoms and clinical findings:
new cognitive impairment
behavioral changes
new focal neurological symptoms
headache (within 6 months of diagnosis; migrainous or oppressive in character)
-
ii. imaging features
rounded T2 hyperintense "snowball lesions"
at least one in the corpus callosum
leptomeningeal enhancement
well demarcated grey matter enhancing on T1 weighted scans
-
-
retinal involvement
i. no clinical findings or symptoms required
-
ii. ophthalmological examinations
branch retinal artery occlusions (BRAO)
arterial wall hyperfluorescence (AWH)
sectorial damage is seen on optical coherence tomography (OCT)
-
vestibulocochlear involvement
-
i. symptoms and clinical findings:
new tinnitus
new hearing loss
new peripheral vertigo
-
ii. examination of inner ear function
audiogram supporting hearing loss
vertigo supported by caloric testing and vestibular evoked myogenic responses
-
A definite diagnosis of Susac syndrome requires fulfillment of all three criteria and their subcriteria, in other words, 1-i, 1-ii, 2-ii, 3-i, and 3-ii.
A probable diagnosis of Susac syndrome can be made if 2 out of the three criteria are met.
Clinical presentation
Susac syndrome classically consists of a clinical triad of:
acute or subacute encephalopathy which could manifest in a broad spectrum of symptoms, e.g. memory impairment, confusion, behavioral disturbances, ataxia, dysarthria, paranoid psychosis, and headaches 1-8
sensorineural hearing loss at low and medium frequencies 1-8
branch retinal artery occlusions (BRAOs) leading to scotomata and vision distortion 1-8, which should be sought by fluorescein angiography 16
At the time of disease onset, the complete triad is only present in a minority of patients (13-27%) 20 and may, in fact, fluctuate over a 1-2 year period, which often leads to a delay in diagnosis 1.
Pathology
The primary pathology is likely to be an autoimmune endothelialopathy (microangiopathy) affecting pre-capillary arterioles, with subsequent embolization, of the brain, retina, and inner ear 1,3,9,19,20. Hence, microinfarcts associated with endothelial proliferation and hypertrophy, basement membrane thickening, and thickening of precapillary arteriolar adventitia with loss of internal elastic lamina 16. Demyelination is not a pathological hallmark of Susac syndrome, in contrast with multiple sclerosis 16.
Markers
Anti-endothelial cell antibodies (AECAs) have been reported as being a promising marker in some studies, but these are not yet considered to be specific to the syndrome 10.
Radiographic features
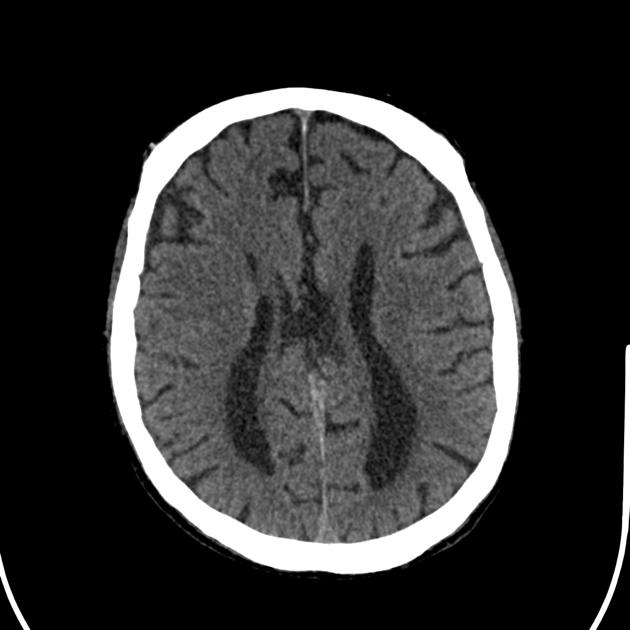
MRI
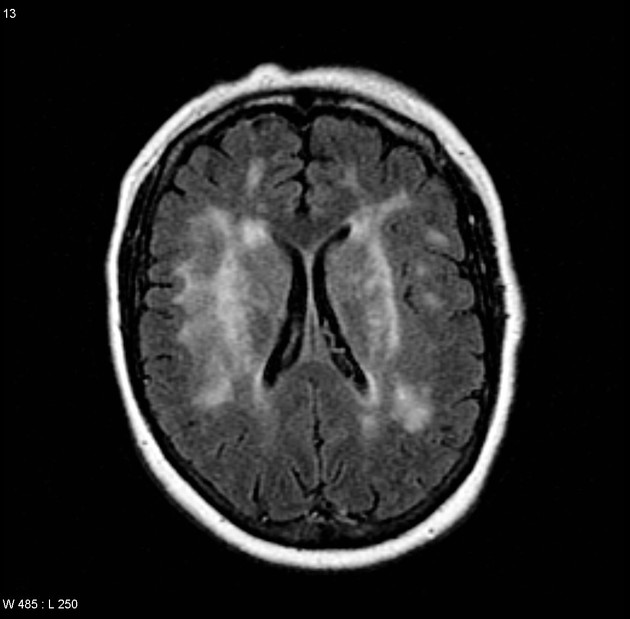
Characteristic radiographic features are present even if all components of the clinical triad have not yet manifested 11. There tend to be multiple, small white matter lesions which have a predilection for the corpus callosum 1,2,8,11.
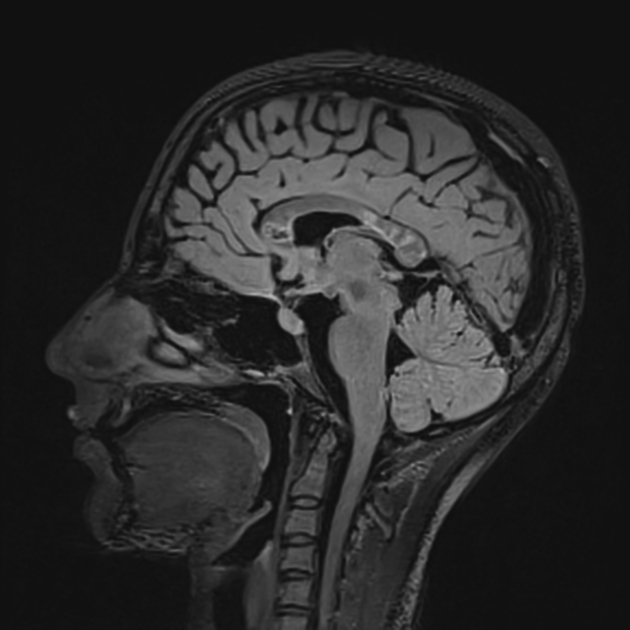
Callosal lesions are considered almost pathognomonic and have many important characteristic features:
typically involve the central fibers of the callosal body and splenium without abutting the callosal undersurface (with relative sparing of the periphery) 1,2,8,11,16
-
lesions are small (3-7 mm) and resembling 16:
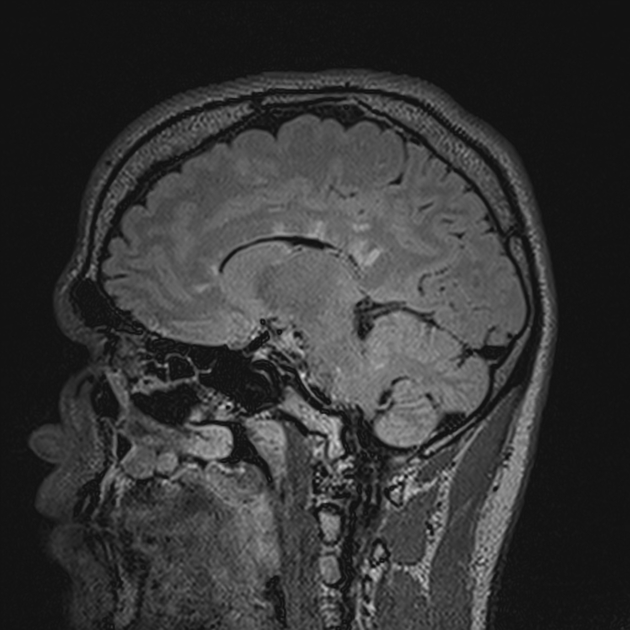
snowball sign on T2 and FLAIR when acute
'punched out' holes on T1 when chronic
lesions, best appreciated on sagittal views, depending on the sequence used 11,12
the roof of the corpus callosum is also frequently involved, rather than the callososeptal interface (which is more typical of multiple sclerosis), resulting in 'icicle' or linear 'spoke' lesions that look to hang from the roof of the corpus callosum 11
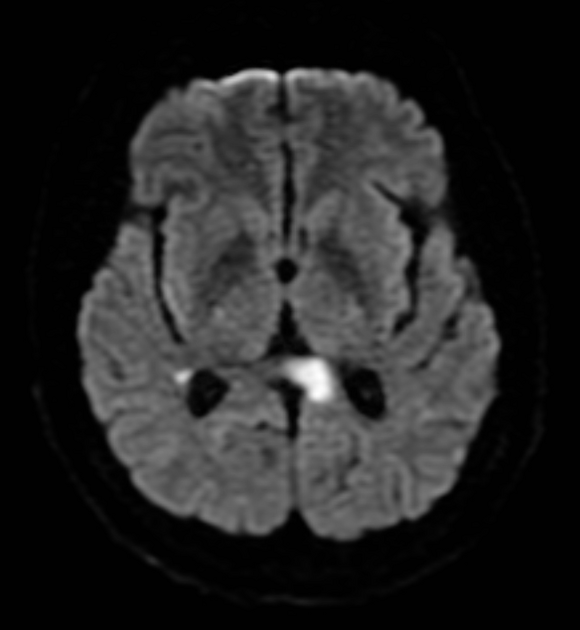
In addition to the corpus callosum, lesions can also involve the periventricular white matter, centrum semiovale, cerebellum, brainstem, and middle cerebellar peduncles 13. A string of pearls sign due to punctate microinfarcts involving the internal capsule has been described 17.
Signal characteristics of all of these lesions include:
T1: lesions are low signal, especially in the chronic stage (see T1 black holes) 1,2,8,11
-
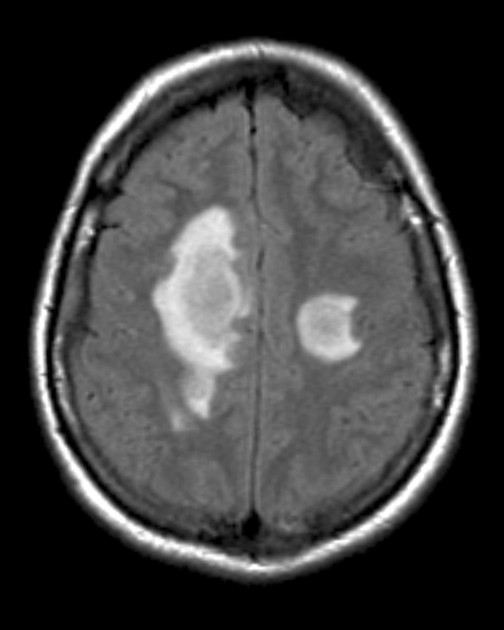
T1 C+ (Gd): lesions frequently enhance during the acute stage 1,2,8,11
there may also be leptomeningeal enhancement independent to lesion location (especially in the cerebellum) 17
T2/FLAIR: lesions are high signal 1,2,8,11
DWI/ADC: high DWI signal, facilitated diffusion 1,2,8
Treatment and prognosis
Although Susac syndrome generally has a monophasic and self-limiting course, case series-level evidence suggests management of the acute episode with immunosuppressants such as prednisolone 14. Intratympanic injection of dexamethasone has also been shown to help with hearing loss, although in severe cases cochlear implants should be considered 6,14. Some patients may have residual neurological sequelae, especially related to retinal infarction 14.
History and etymology
The disorder was initially described by John O Susac (1940-2012), an American neurologist and neuro-ophthalmologist, and his colleagues in their 1979 seminal paper on two patients with the classic clinical triad 3. The eponym was famously first used in 1986, when a patient was presented in a neuro-ophthalmology conference with the same triad that Susac et al. had described, prompting one member of the conference to exclaim “this is Susac’s syndrome” 15.
Differential diagnosis
Other entities can produce a similar MR appearance:
-
demyelinating conditions
-
multiple infarcts caused by
thromboembolic disease
-
systemic lupus erythematosus (SLE) related vasculitis
transient lesion of splenium of corpus callosum: shows restricted diffusion and no enhancement


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.