
Temporal encephaloceles are usually small encephaloceles, often asymptomatic, but increasingly recognized as potential causes of refractory epilepsy and as a sequela of idiopathic intracranial hypertension.
On this page:
Epidemiology
Temporal encephaloceles can be congenital or secondary to trauma, idiopathic intracranial hypertension or prior surgery. As such, the demographics of affected individuals are heterogeneous and correlate with etiology. In the setting of refractory epilepsy, the incidence has been reported to be 2-4%, higher in temporal lobe epilepsy 1.
Clinical presentation
The majority of small temporal encephaloceles are probably asymptomatic, although true incidence of symptoms is uncertain as they are difficult to identify on routine imaging. When symptomatic they most commonly present as a focus of refractory temporal lobe epilepsy or CSF rhinorrhea. In many individuals, the presenting symptom will be due to idiopathic intracranial hypertension and the encephalocele discovered during assessment for headaches.
Importantly, base of skull encephaloceles with CSF leak rarely, if ever, present with signs and symptoms of intracranial hypotension 4,5.
Radiographic features
MRI
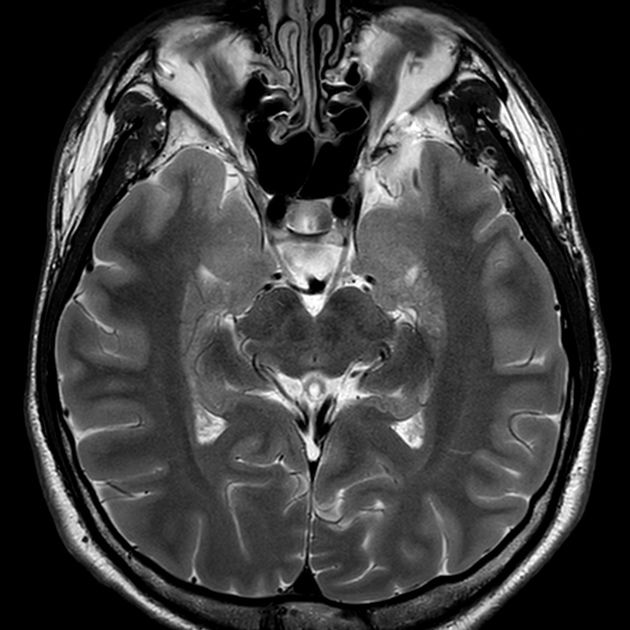
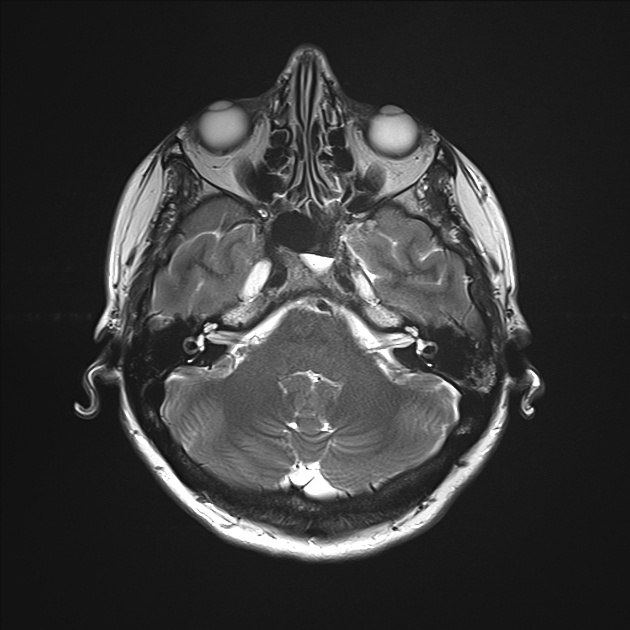
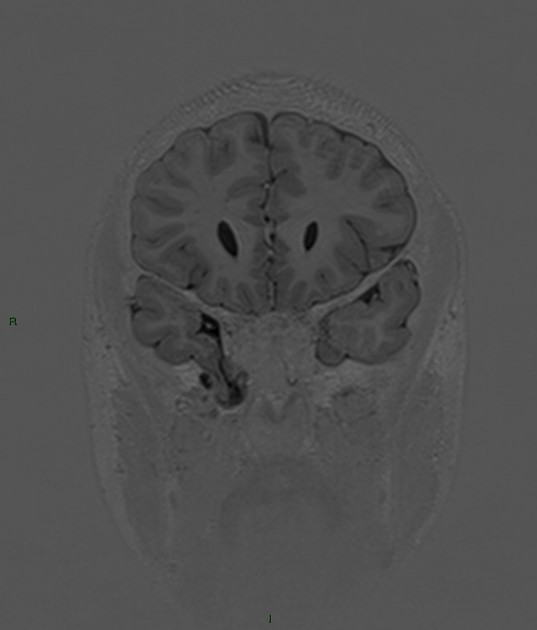
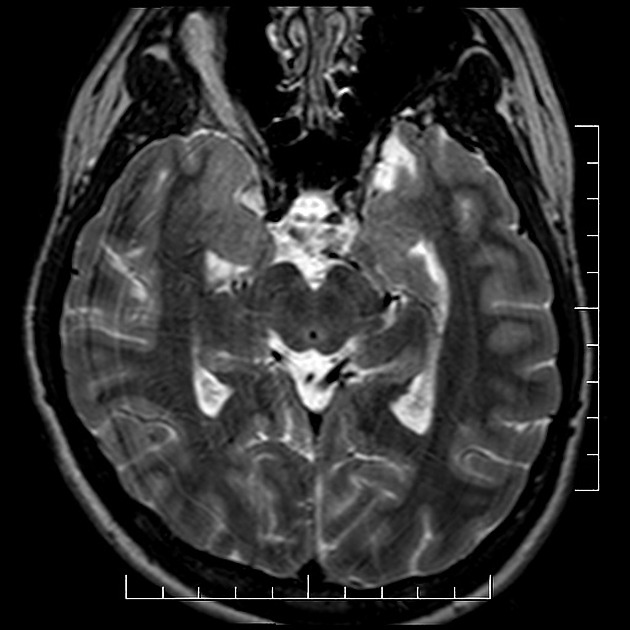
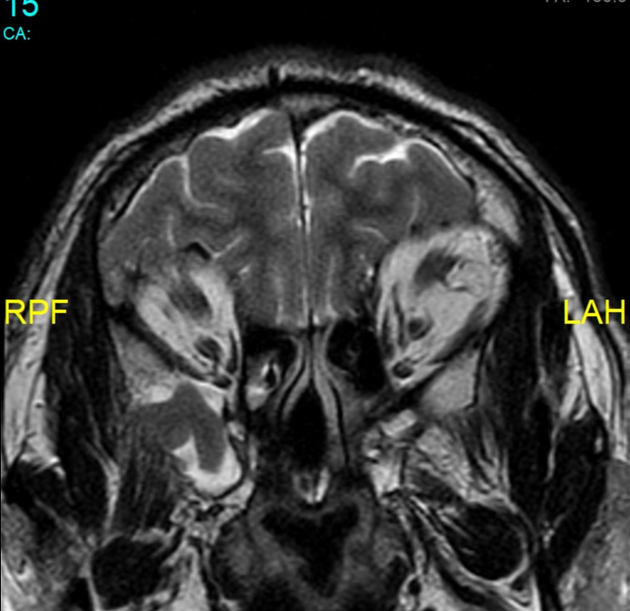
A good quality MRI with dedicated thin or volumetric T1 and T2 weighted sequences is essential in adequately visualizing small temporal encephaloceles 1.
They are frequently (two-thirds) bilateral and most frequently involve the anteroinferior temporal lobe through the floor of the middle cranial fossa 1. In some instances, focal herniation of the posterior inferior temporal gyrus occurs into an arachnoid granulation protruding into a dural venous sinus 2,3. It is unclear, however, if these are also the cause of refractory epilepsy.
Treatment and prognosis
In individuals with refractory temporal lobe epilepsy, and especially if seizure activity can be localized to the encephalocele, then surgical resection and repair have good clinical outcomes 1.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.