
Transsphenoidal hypophysectomy, also known as endoscopic transsphenoidal surgery (ETSS), is a commonly used surgical approach for pituitary region masses, with many significant advantages over open craniotomy.
On this page:
Images:
History
The transsphenoidal approach was first described in 1907 by Schloffer, modified by Halstead and subsequently popularized by Harvey Cushing, who is most associated with this technique 2. It is interesting to note that towards the end of his career Cushing abandoned transsphenoidal surgery in favor of a subfrontal approach 2,3.
Indications
Transsphenoidal surgery is indicated in many pituitary region tumors, including:
-
pituitary adenomas
pituitary macroadenomas provided they are mostly midline
craniopharyngiomas (provided they are intrasellar)
biopsy of midline sphenoclival lesions (e.g. chordoma, aspergilloma, meningioma etc.)
debulking of larger tumor
It is important to note that the size of the suprasellar component is not terribly important, and tumor can be delivered down into the pituitary fossa from as high up as the foramen of Monro 1. This can be aided by Valsalva maneuver or introduction of air or sterile saline via a lumbar drain.
Contraindications
The main limitation of the transsphenoidal approach is that the operative corridor is narrow and lateral tumor is difficult to resect. As such tumors with large parasellar components should be tackled transcranially if a total resection is being aimed for 1.
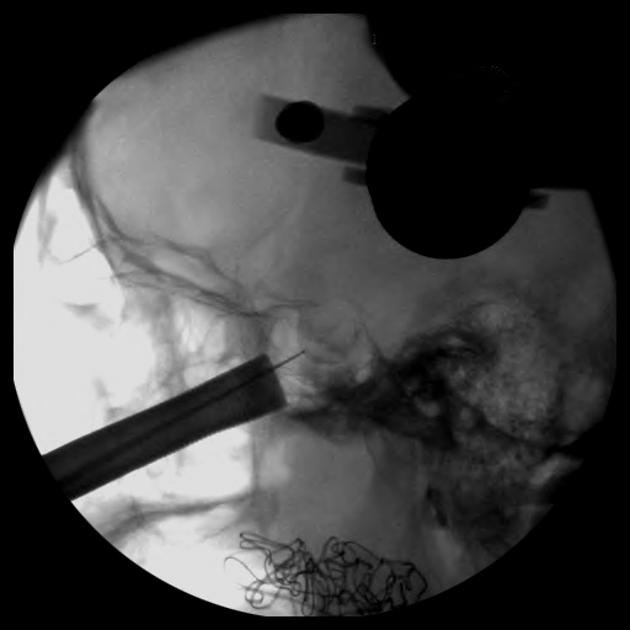
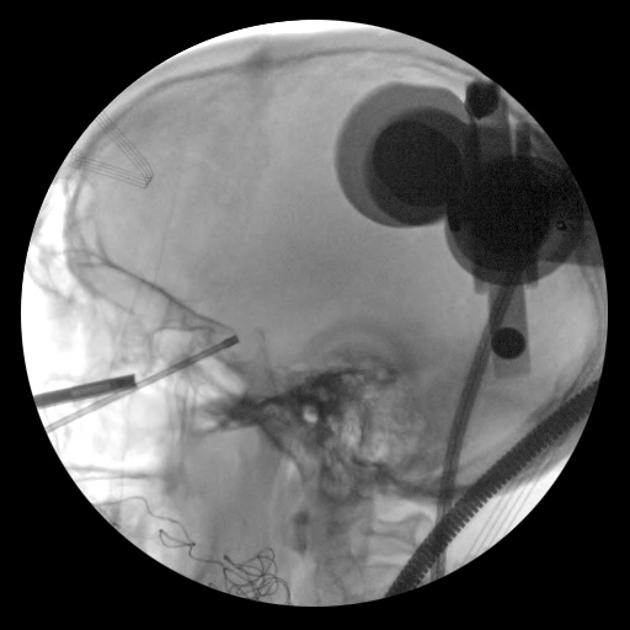
Procedure
It is beyond the scope of this article to go into operative details, and only a brief summary is provided, at a level useful to a radiology audience 1.
general anesthesia
patient is placed semi-sitting in Mayfield tongs
intraoperative fluoroscopy is used to confirm instrument positioning
operative microscope is used
incision in the buccal mucosa under the upper lip
blunt submucosal dissection along the nasal septum to the sphenoid sinus
speculum inserted
anterior wall of the sphenoid sinus is opened
mucosa of the sphenoid sinus is removed from the posterior wall
anteroinferior wall of the pituitary fossa is opened
the dura is opened
tumor is removed with a variety of instruments (e.g. pituitary rongeurs)
the surgical defect is packed with fat
anterior wall of the fossa reconstituted with bone/cartilage/glue etc.
further fat packing
nose is packed with petroleum jelly (e.g. Vaseline) gauze impregnated with bacitracin ointment
lip incision closed
Endoscopic techniques have also been developed.
Complications
Complications include:
postoperative hemorrhage presenting similarly to pituitary apoplexy
CSF leak which may result in meningitis


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.