
Presentation
Acute abdominal pain for the past three days. Patient has a history of prior episodes of hematochezia and hemoptysis.
Patient Data
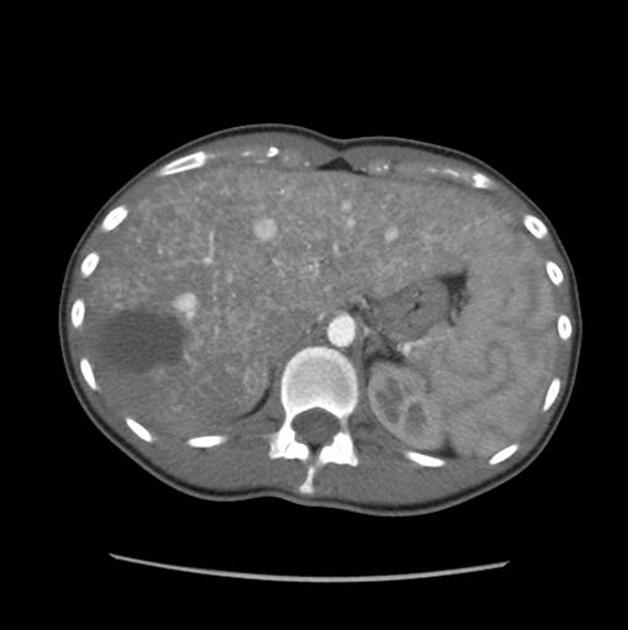
Heterogeneous enhancement, prominence of the hepatic artery, early filling of dilated hepatic veins, small telangiectasias, and a focal necrotic low density area in the posterior segment.
Due to persistent pain, the patient subsequently underwent a posterior wedge resection.

Slight tortuosity of dilated hepatic arterial branches. Numerous irregular areas of dense contrast accumulation throughout the liver parenchyma with a mottled capillary blush and early filling of hepatic veins.
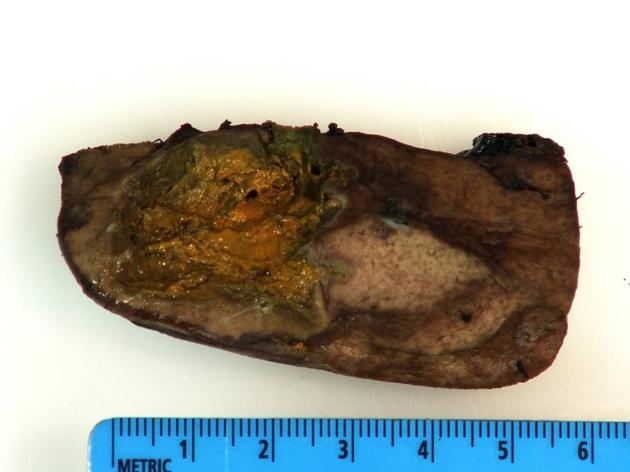
Confluent necrosis with focal bile extravasation. The background liver demonstrated multiple telangiectasias consistent with hereditary hemorrhagic telangiectasia (HHT).
Case Discussion
Symptomatic liver involvement in HHT is uncommon but does occur. It has been attributed to three distinct clinical subtypes and is believed to be a consequence of the predominant hepatic shunt pattern:
- high-output cardiac failure
- shunting that increases cardiac preload
- typically arteriovenous or portovenous shunts
- portal hypertension
- increased flow into the portal system (arterioportal shunt)
- hepatic anatomic abnormalities leading to increased intrahepatic resistance
- biliary disease
- shunting of the blood away from the peribiliary plexus (arteriovenous or arterioportal shunting)
- our case – extensive arteriovenous shunting lead to biliary necrosis and bile leak


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.