
Presentation
Polytrauma patient.
Patient Data
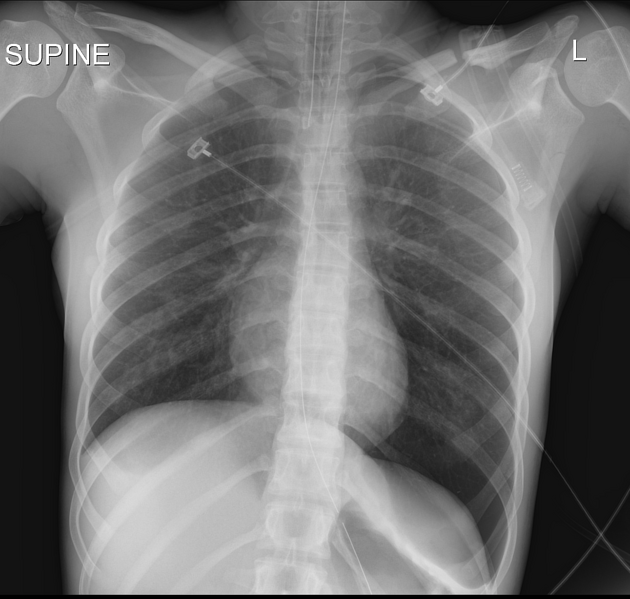
Endotracheal and nasogastric tubes are appropriately positioned. Minimal left basilar opacity likely due to pulmonary contusion, lungs otherwise clear. Lucent left diaphragm and left deep sulcus sign indicating left pneumothorax. Left clavicle fracture.

New left chest tube appropriately positioned with resolution left pneumothorax.
Case Discussion
When patients are upright, pleural air gathers at the lung apices, resulting in the familiar apical visceral pleural line of a pneumothorax. But in the supine position, air in the pleural space accumulates anteriorly and inferiorly: this is the least dependent part of the chest in the supine position. Air projecting over and lateral to the diaphragm results in increased lucency of the diaphragm and deepening of the lateral costophrenic sulcus. The deep sulcus sign may be the only finding of a pneumothorax in a supine patient.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.