
Presentation
Lower abdominal pain, more on right. Raised inflammatory markers despite having been on cefuroxime for several days for a urinary tract infection. No fever or shivers.
Patient Data




The cecum curves upward, wherefore the appendix originates cranial to the ileocecal valve.
Normal-appearing mediocecal appendix, its distal part bordering the liver.
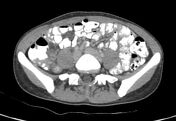
Single diverticulum on the mesenteric border of the terminal ileum, approximately 2 cm from the ileocecal valve, surrounded by mesenteric fat stranding which contains a couple of tiny gas bubbles. Several reactive mesenteric lymph nodes nearby. The terminal ileum is thickened.
Case Discussion
Ileal diverticulitis with perforation in a young woman, a very rare diagnosis. It is quite possible that had she undergone ultrasound imaging, the diagnosis would have been delayed.
She received antibiotic treatment and recovered uneventfully.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.