
Presentation
Pain in left clavicle.
Patient Data



A large lytic and expansile lesion involves the medial third of the clavicle.

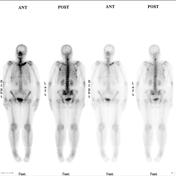
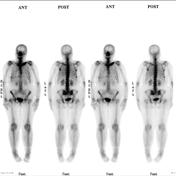
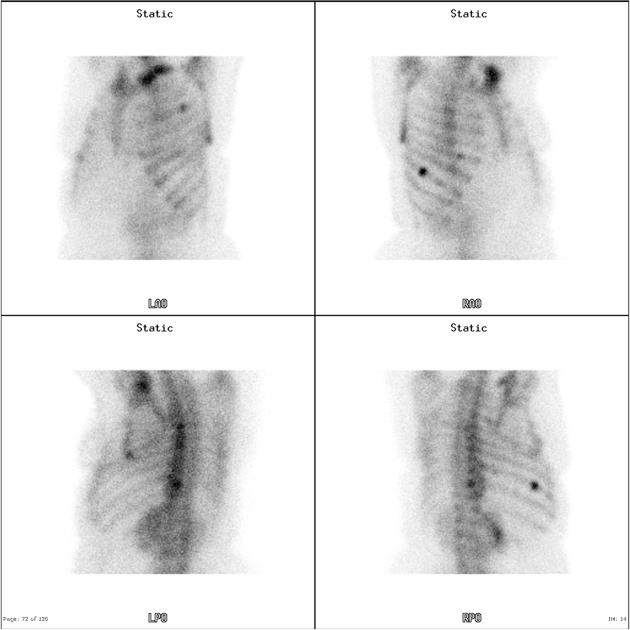
The study shows increased tracer uptake consistent with osteoblastic bony metastases in left clavicle, proximal part of the left humerus, inferior part of the left sacroiliac joint, T11 vertebral region, T7 and T8 vertebral region, mid-cervical spine, right 8th and 9th ribs laterally.


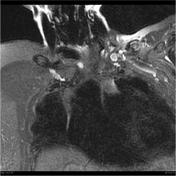
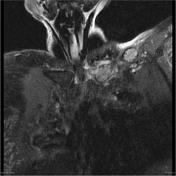
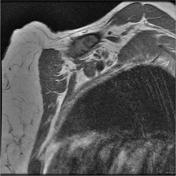

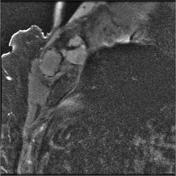
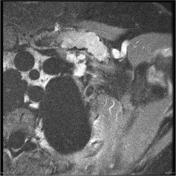

An expansile multilobulated intramedullary, T1 hypointense, heterogeneous T2 hyperintense enhancing lesion extends from the medial aspect of the clavicle to involve the shaft for a length of approximately 7 cm. The lesion is expansile with evidence of cortical erosion and cortical breach with a small ( 6mm) soft tissue component protrudes through the posterior cortex of the clavicle. No convincing periosteal reaction. There is a wide zone of transition along the lateral aspect of the lesion. No extension into the manubriosternal articulation. No encasement of the adjacent subclavian vessels.

Under CT guidance, following lignocaine local anesthetic and IV Meperidine 50mg, via a 13g coaxial needle, six 14g core biopsies of the left clavicle mass were obtained. No immediate complications.
Histology
Five rubbery pale tan/red fragments up to 6mm in greatest dimension.
MICROSCOPIC DESCRIPTION: The vascular fibrofatty and muscular tissue shows a few small foci of poorly cohesive malignant cells some of which show a signet ring cell appearance.
- Immunostaining for her2 oncogene product is negative.
- Ecadherin staining shows weak focal staining interpreted as non specific and negative.
- Estrogen receptor: postive
- Percentage of nuclei stained: >95
- Predominant intensity of staining: strong
- Progesterone receptor: postive
- Percentage of nuclei stained: >95
- Predominant intensity of staining: strong
FINAL DIAGNOSIS: Left clavicular biopsy: Metastatic carcinoma consistent with a primary lobular breast cancer.

Distribution of skeletal metastases. Layout and distribution: Frank Gaillard 2012, Line drawing of skeleton: Patrick Lynch 2006, Creative Common NC-SA-BY
Case Discussion
This case illustrates a relatively atypical skeletal metastasis from breast cancer.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.