
Presentation
Upper limb weakness increasing over a number of weeks with increased tone in legs.
Patient Data





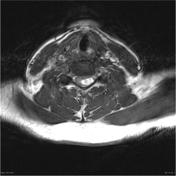



An enhancing nodule is present within the cord at the level of C5 with adjacent peritumoural cysts and extensive cord edema. Posterior to the lesion a number of serpentine flow voids are noted. The mass has evidence of blood products (previous hemorrhage) and vivid enhancement.



A central vividly enhancing mass (green arrows) is surrounded by cystic elements and has a prominent serpiginous flow void posteriorly (red arrow). The entire cord is edematous, and the peritumoural cists are lined by hemosiderin (blue arrow)
MICROSCOPIC DESCRIPTION: Paraffin sections show a moderately hypercellular, intensely vascular tumor. This is composed of cells with moderately pleomorphic round oval and angulated hyperchromatic nuclei and a variable amount of pale and foamy cytoplasm. These are arranged in diffuse sheets as well as lobules which are enclosed by thin-walled capillaries. Vascular spaces vary from large caliber thin-walled sinusoidal structures to capillaries. A very occasional mitotic figure is identified in tumor cells. No areas of necrosis are seen. Tumor is attached to dense collagenous tissue consistent with meninges.
Immunohistochemistry shows strong staining of vascular endothelium for CD34. No reactivity for GFAP, CD34 or cytokeratrin AE1/AE3 is seen in tumor cells. The features are of capillary hemangioblastoma.
FINAL DIAGNOSIS: Capillary hemangioblastoma.
Case Discussion
This patient went on to have screening of the rest of the neuraxis and of the kidneys and there was no sign of other lesions. Screening for vHL was negative.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.