
From the case:
Total anomalous pulmonary venous return (type I)


Download
Info
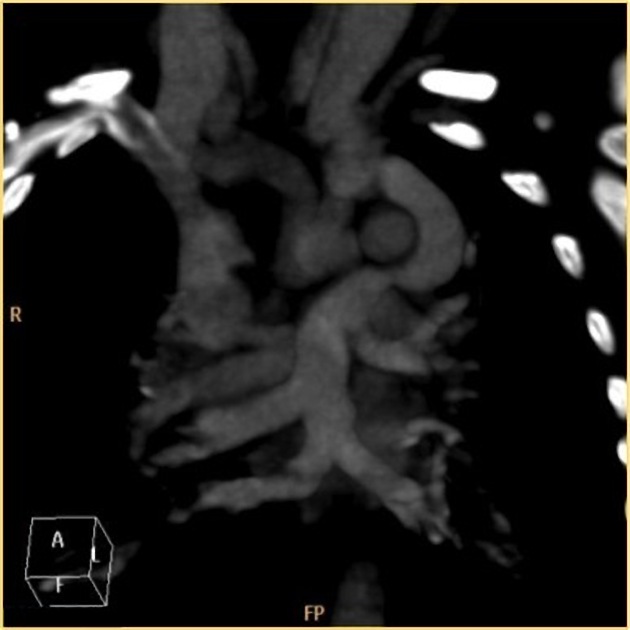
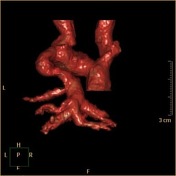
All pulmonary veins drain into the superior vena cava through the left vertical vein and left brachiocephalic vein.
Case Discussion
The current case represents type I (supra cardiac) total anomalous pulmonary venous return (TAPVR), which is the most common type and accounts for 55% of cases. The common pulmonary venous sinus drains into the right superior vena cava (SVC) through the left vertical vein and left brachiocephalic vein. An interatrial communication (right-to-left shunt), either an atrial septal defect (ASD) or patent foramen ovale (PFO), is necessary for survival.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.