
Presentation
Bilateral flank pain, dysuria, fever, and laboratory findings are suggestive of septicemia.
Patient Data

Inflammatory changes are seen related to the whole urinary tract in the form of fluid collection and stranding of the surrounding fat planes, starting from both kidneys down with the ureters to the prostate, seminal vesicles, and urinary bladder. The process seems to be more profound in the pelvis. The prostate is markedly swollen with hypodense hypoenhancing parenchyma. The seminal vesicles also appear congested and swollen. The urinary bladder shows diffuse wall thickening and edema. There is also a bilateral retroperitoneal fluid collection. There are some motion artefacts as the patient was distressed and irritable.
Overall the picture is of a disseminated urinary tract infection with prostatitis, seminal vesiculitis, and cystitis.


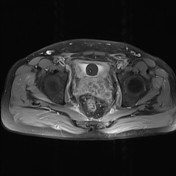

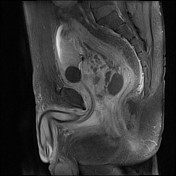
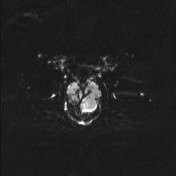
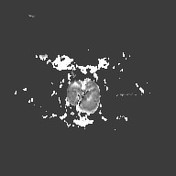
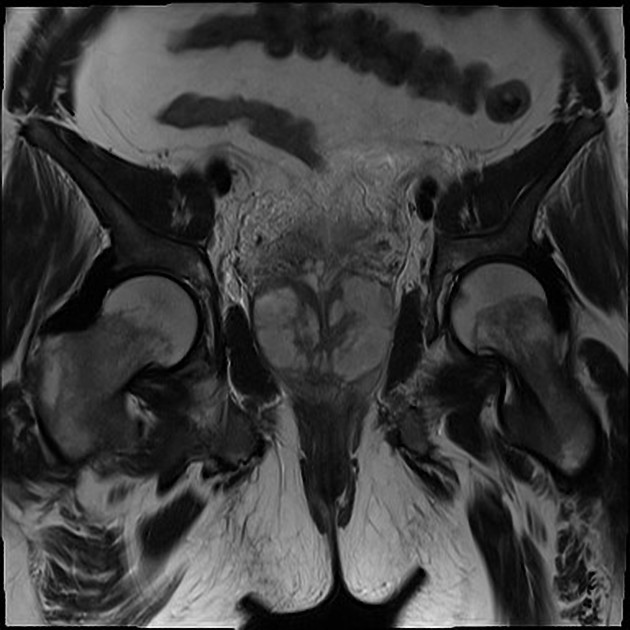
Follow-up MRI done after around a week. No drainage was done. The patient was on a high dose of broad-spectrum antibiotics. The prostate is currently more irregularly enlarged and shows frank pockets of fluid collection and with enhancing walls which showed restriction on DWI and diminished ADC values confirming the inflammatory nature of the process. Similar changes are also noted in the seminal vesicles. However, the urinary bladder seems to show some regression of the wall edema and thickening in comparison to the previous CT.
Case Discussion
Extensive urinary tract infection involving the kidneys down to the urinary bladder, seminal vesicles and prostate. The changes seemed to be more severe at the prostate and seminal vesicles with diffuse congestion and related fluid collection and fat stranding. Follow-up MRI showed evident breaking down (fluid signal) within the prostate with enhancing septations, suggesting frank prostatic abscess formation, which is confirmed by the diffusion restriction seen within these pockets. Milder similar changes are also seen at the seminal vesicles.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.