
Presentation
One year history of central hypothyroidism of unknown etiology.
Patient Data


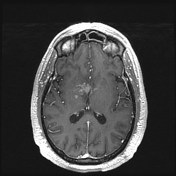
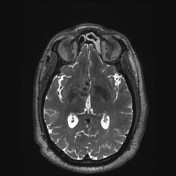
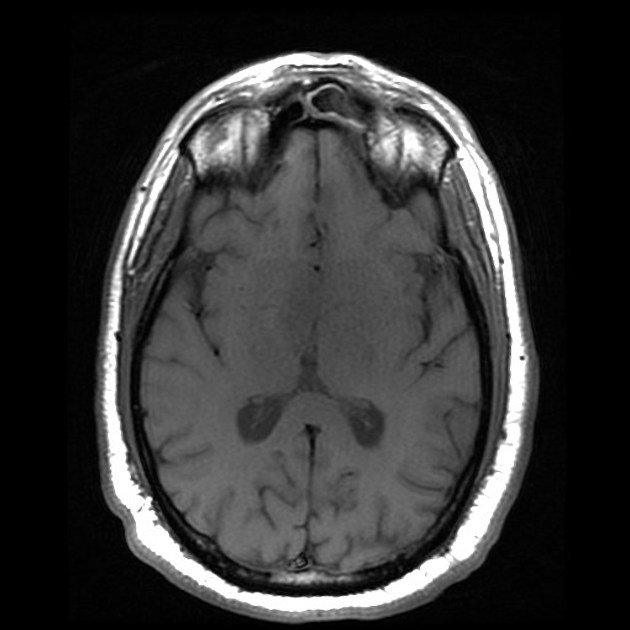
Centered within the right greater than left thalamus/hypothalamus, there are multiple ill-defined punctate and ringlike foci of enhancement with T2 hypointense signal. These areas are surrounded by patchy, minimally expansile T2 hyperintensity throughout the anterior perforated substance, hypothalamus, optic tracts, internal capsules, putamina and ventral thalami.
Case Discussion
This is a biopsy-proven case of hypothalamic amyloidoma. Differential considerations for this appearance would include a granulomatous process such as neurosarcoidosis, infection or an atypical appearance of CNS lymphoma.
Amyloid deposition within the brain can take many forms, including cerebral amyloid angiopathy, senile plaques of Alzheimer dementia, deposits seen in the encephalopathy of Kuru and of Creutzfeldt-Jacob disease, or tumor-like focal deposits known as amyloidomas. The latter is the most rare form of cerebral amylodosis, with only a small number of case reports in the literature.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.