
Presentation
50 year old with a previous thoracic condition, presents for follow up.
Patient Data


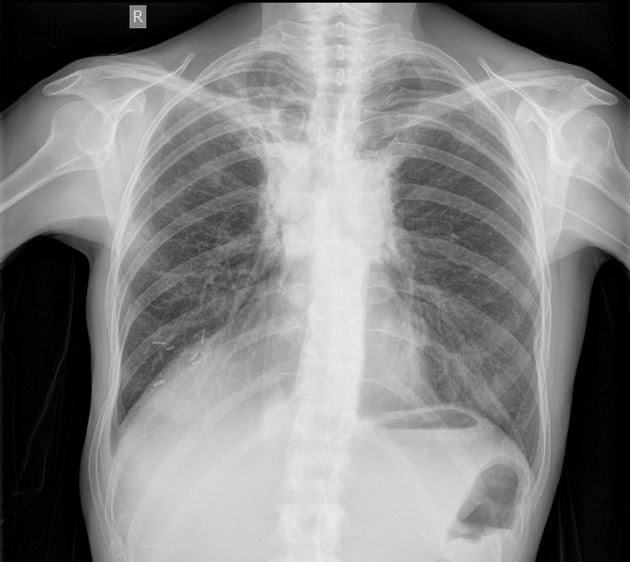
Chest Xray:
- Evidence of right mastectomy
- Elevation of right hemidiaphragm
- Bilateral perihilar and paratracheal opacities
- Streaky opacities in the right upper lobe
- Area of rounded lucency projected over the medial aspect of the right clavicle
- Indistinct outline of the left side of the body of T6
- Left sided PICC line, satisfactorily positioned



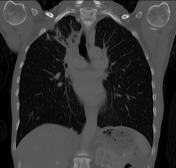
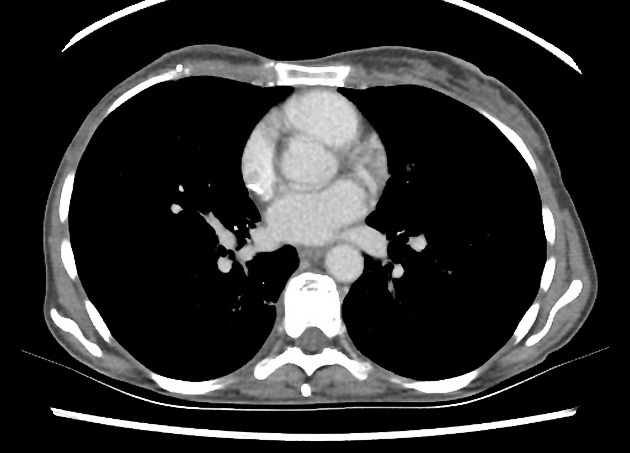
CT Chest (axial C+, lung window and coronal bone):
- Irregular thick-walled cavitating lesion in the right upper lobe
- Scattered 4-6mm pulmonary nodules in the right upper lobe
- Dense air-space opacity in both upper lobes in paramediastinal distribution with sharply defined linear outer borders, traction bronchiectasis
- Air-space opacity in the right upper lobe
- Soft tissue density mass anterior to the left side of the heart
- Scattered vertebral body lytic lesions throughout the visualized axial skeleton, compression of the left side of the body of T5
Case Discussion
This is an excellent case for the film viewing component of the FRANZCR part 2 examination. A constellation of findings lead to multiple pathology in this study, all related to the underlying diagnosis of right breast cancer.
1. A cavitating lesion in a patient with history of breast carcinoma carry two main considerations: cavitating metastasis or fungal infection. The mnemonic that helps one to remember the differentials of a cavitating lung lesion is:
T I G S
T = Tumor (primary such as SCC, secondary such as TCC, sarcoma etc), I = Infection (abscess, fungal etc), G = Granulomatous inflammation (Sarcoid, Silicosis, Rheumatoid arthritis, Wegener granulomatosis), S = Septic emboli
2. Multiple pulmonary nodule in this patient can be due to fungal infection or metastatic spread.
3. Typical findings of radiation induced fibrosis (dense paramediastinal consolidation along the radiation field, traction bronchiectasis and sharply delineated lateral margins).
4. Extensive skeletal metastases


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.