
Presentation
Tenesmus.
Patient Data


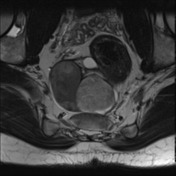
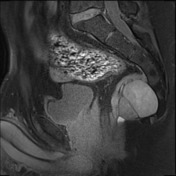
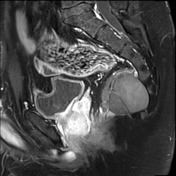
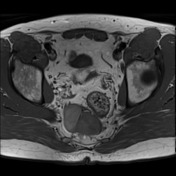
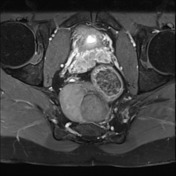
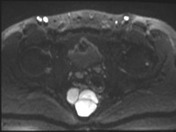


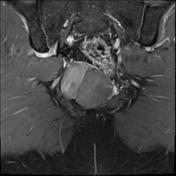
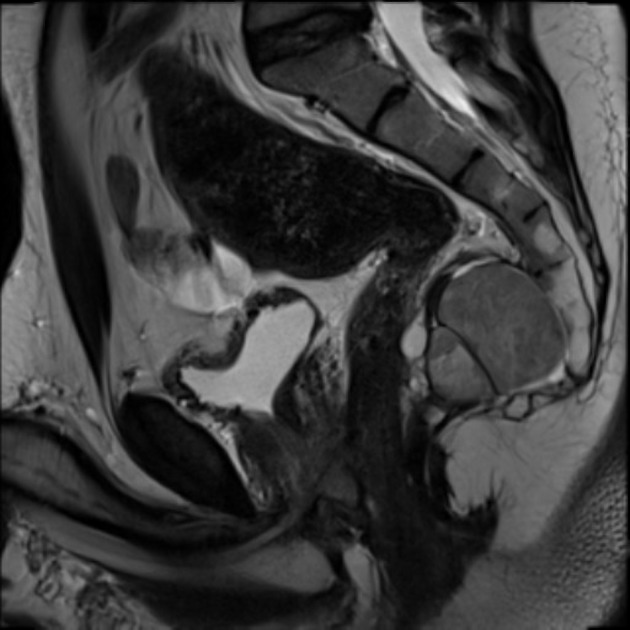
There is a presacral mass which extends into the pelvic floor - midline and slightly right-sided. The cyst contains multiple tiny and large cystic elements ranging from 5 - 43mm. There is no significant enhancement or solid elements. The rectum and anal canal are displaced but otherwise normal. This lies intimate relationship with Waldeyer's fascia (rectosacral, and this fascia limits the tumor superiorly). Inferiorly, the tumor is clear of the levator ani. The prostate is deeply grooved midline posterior surface in the peripheral zone which has abnormal signal. No other discrete mass is seen. The prostate is moderately atrophic. The prostate findings are presumably congenital in nature and of uncertain significance.
The sacrum is mostly normal with its most distal segment on the left hypoplastic and dysplastic curved coccyx.
Conclusion: Posterior pelvic floor complex cystic mass with benign features has an imaging appearance consistent with an epidermoid. A cystic teratoma is less likely (only considered on genetic grounds; epidermoid favored on imaging grounds).
Case Discussion
Family history of Currarino syndrome. This individual is MNXI gene mutation positive.
Case courtesy do A.Prof Damien Stella.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.