
Presentation
Past medical history of tuberculosis (TB) treated in 2013, presenting with cough, fatigue and one episode of hemoptysis. Chest x-ray evaluation for recurrent tuberculosis.
Patient Data


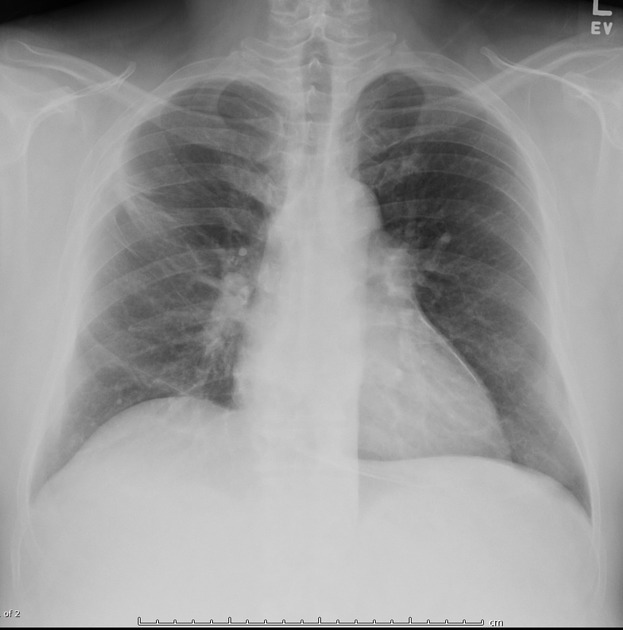
No new focal pneumonia, effusion or pneumothorax. Mild diffuse bilateral peribronchial thickening.
Stable right upper lobe scarring with adjacent pleural thickening/reaction consistent with history of tuberculosis. No evidence of active TB.
The heart remains normal sized without pulmonary vascular congestion.
Almost diffuse curvilinear/circumferential pericardial calcification.
No acute osseous findings.
Case Discussion
Tuberculous pericarditis is frequently reported as the primary cause of pericardial calcification 1 and occurs in approximately 1 to 2 percent of patients with pulmonary tuberculosis (TB). This is a rare finding in the Western World. However, tuberculous pericarditis accounts for nearly 10% of chronic constrictive pericarditis cases in the United States 2. There is strong evidence that large calcific pericardial deposits indicate “burnt-out” pericardial tuberculosis 2. Detecting the pericardial calcification on radiography is important for definitive diagnosis 2.
The differential diagnosis for pericardial calcifications include 1:
- idiopathic
- viral
- TB
- trauma
- cardiac surgery
- radiation
- connective tissue disorders
- malignancy
This case was submitted with supervision and input from:
Soni C. Chawla, M.D.
Associate Professor
Department of Radiological Sciences
David Geffen School of Medicine at UCLA
Olive View - UCLA Medical Center


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.