
Presentation
Polydipsia, polyuria, oral and skin lesions for 4 months. Hormonal measurements showed hypogonadism, hypothyroidism and panhypopituitarism.
Patient Data
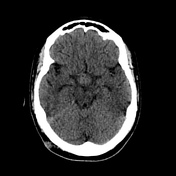


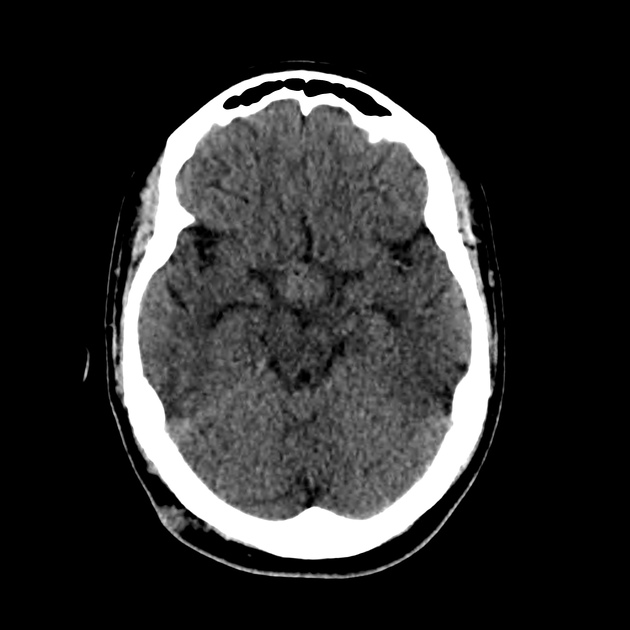
Non-contrast CT brain shows a suprasellar hypodense mass lesion, best seen in the sagittal reconstruction.
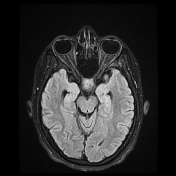
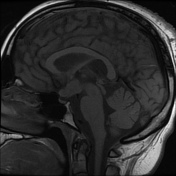
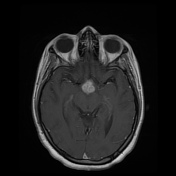
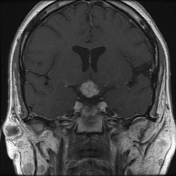
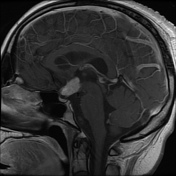
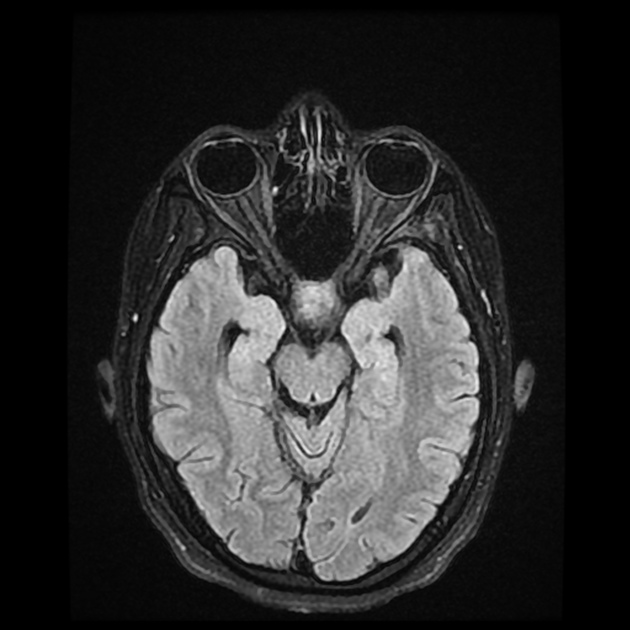
MRI images show a suprasellar mass lesion with hypointense signal on T1-weighted imaging and hyperintense signal on T2-weighted imaging with intense contrast enhancement and thickness of pituitary stalk. Note the loss of the normal posterior pituitary bright spot.
Case Discussion
WHO classify histiocytic disorders into three groups: dendritic cell disorders, macrophage-related disorders, and malignant histiocytic disorders. Langerhans cell histiocytosis (LCH) is part of dendritic cell disorder.
In LCH, the CNS involvement is rare but is potentially devastating. The most frequent clinical CNS manifestation of LCH is diabetes insipidus secondary to infiltration of the posterior pituitary gland.
CNS complications of LCH include mass lesions and a neurodegenerative syndrome. The most common CNS manifestation in LCH is infiltration of the hypothalamic-pituitary region by LCH granuloma, frequently leading to diabetes insipidus which results in decreased secretion of antidiuretic hormone. T1-weighted MR imaging demonstrates loss of the normal posterior pituitary bright spot. Some patients show thickening of the pituitary stalk.
Neurodegenerative changes, the second most frequent pattern, comprise mostly symmetric lesions in the cerebellum and basal ganglia.
Intra-axial mass lesions are the least common CNS manifestation of LCH. Less frequently, there may be mass lesions in the extra-axial spaces, such as the meninges, pineal gland, and choroid plexus.
The treatment regimens for CNS LCH included prednisone, vinblastine, etoposide, cladribine and intravenous immunoglobulin. Irradiation also is used in some cases.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.