
Presentation
Patient admitted to the hospital with a few history of abdominal colicky pain, distension, and vomiting.
Patient Data
Age: 65 years
Gender: Female
From the case:
Cecal volvulus



Download
Info

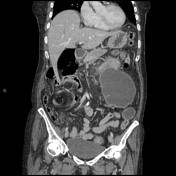
Coronal images from the CT abdomen and pelvis show the cecum displaced into the left upper quadrant, with mesenteric fat and vascular swirling along the ascending colon. The stomach is collapsed.
Case Discussion
Cecal volvulus is caused by axial twisting of the cecum along with the terminal ileum and ascending colon with large bowel obstruction. If untreated, cecal volvulus can progress to bowel ischemia, necrosis, or perforation. In most patients with cecal volvulus, the torsion is located in the ascending colon above the ileocecal valve.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.