
Presentation
Left pleuritic chest pain. 4 weeks post admission for pneumonia and pleural effusion.
Patient Data



WIthin the left midzone is a retained horizontal fragment of catheter tubing. No residual pleural effusion. Chronic interstitial thickening is longstanding. Cardiomegaly. Evidence of prior CABG.
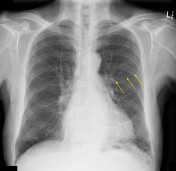

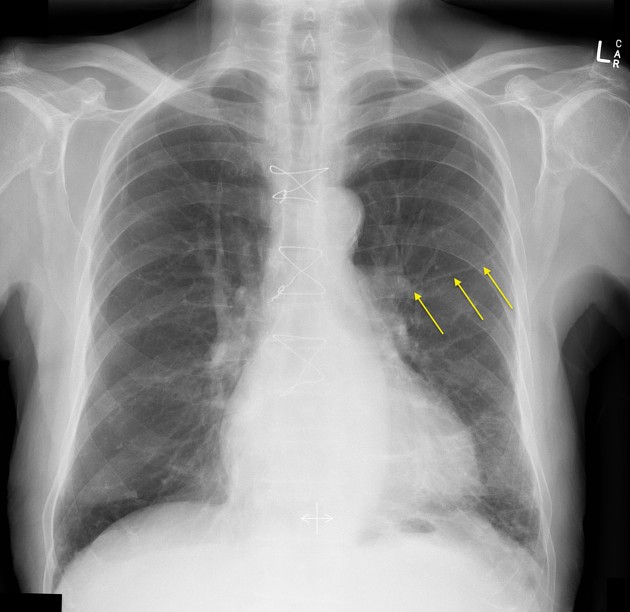
Annotated position of the retained segment of pleural catheter tubing.
Case Discussion
The patient had a LLL pneumonia (CXRs not available) requiring IV antibiotics a month earlier complicated by a moderate-sized left pleural effusion. The effusion was treated with a pleural catheter (aspirate was sterile serous fluid) and the catheter was inadvertently dislodged overnight 3 days after insertion when the patient was delirious. The catheter was thrown away without inspection by the night staff.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.