
Presentation
Abdominal pain.
Patient Data




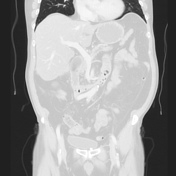

The cecum is dilated and twisted 180 degrees counterclockwise, flipped cranially and midline. The axis of rotation is best seen on axial images, and the inverted relationship with the terminal ileum is best seen on the coronal reformats (lung and standard). Also, see the annotated images. A small amount of edema surrounds the cecum.
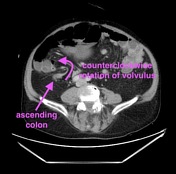
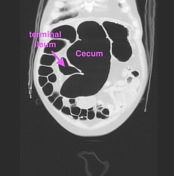

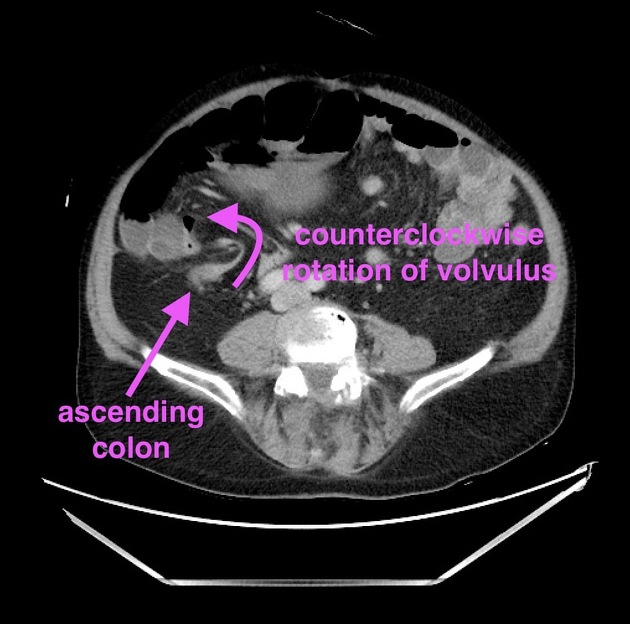
Annotated images show key observations to help understand the anatomy.
Case Discussion
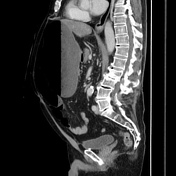
Cecal volvulus which was managed with urgent surgery and right hemicolectomy. Colonic volvulus can be challenging to follow on CT, and at times it is helpful to look at the scout images, which in this case has the fairly typical appearance of dilated colon flipped up into the upper/mid-abdomen.
The key to making sense of the anatomy in cases of colonic volvulus is to find a segment of normal colon and try to follow it into the volvulus. In this case, start at the rectum -> sigmoid -> descending -> decompressed and distorted transverse -> finally the ascending, which leads into the volvulus. In order to confirm the diagnosis, find the inverted TI (coming from the lateral cecum rather than medially) on the coronal images - the annotated images show the relationship.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.