
Presentation
4 weeks history of epigastric pain, admitted 2 weeks ago with elevated lipase (1220 units/L).
Patient Data


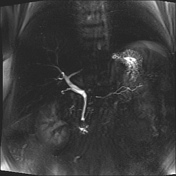
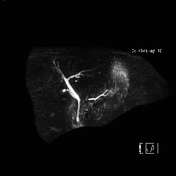
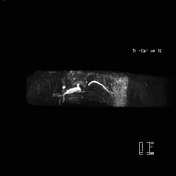
Status post cholecystectomy with residual 7 mm thin-walled cyst adjacent to the cystic duct stump. No biliary tree dilatation or filling defects to suggest intraductal stones.
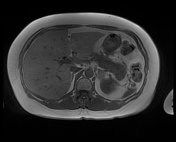
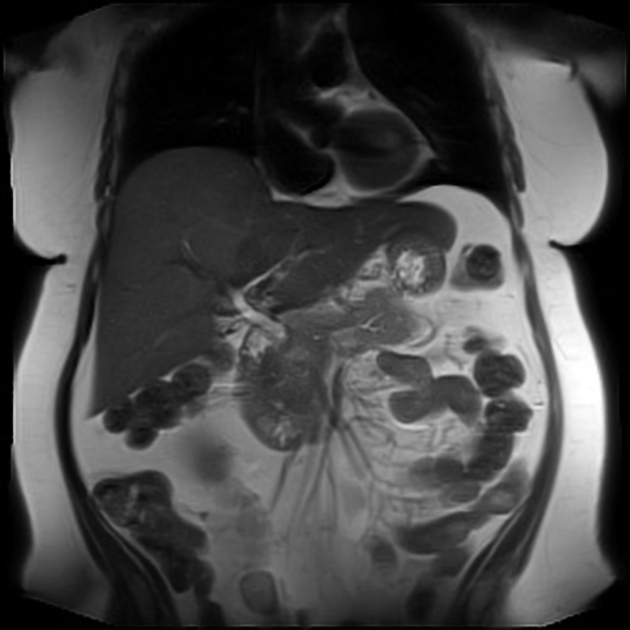
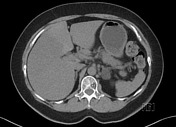
There few small simple hepatic cysts in segments six and seven. The liver has a diffuse drop of the signal on T1 out of phase, in keeping with steatosis.
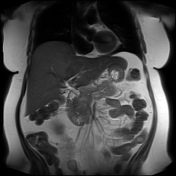
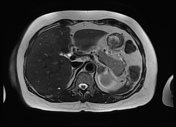
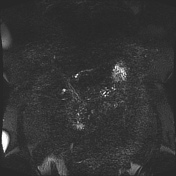
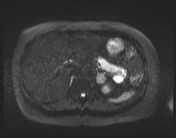
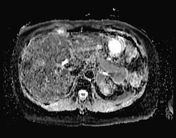
There is a cutoff of the main duct at the level of the pancreatic neck, with mild upstream duct prominence (2 mm). An ill-defined rounded area measuring about 2 cm shows a slightly increased T2 signal at the pancreatic head, close to the cutoff of the main duct. Mildly diffuse elevated DWI signal and increased pancreatic bulkiness. No peripancreatic collections or discrete inflammation.
Left adrenal gland adenoma stable when compared to CT from 10 years ago (not shown). The right adrenal gland, kidneys, and spleen are normal.
An ill-defined pancreatic head lesion with a sudden cutoff of the main duct is highly concerning for an underlying adenocarcinoma. In the setting of recent pancreatitis episode, distortion related to pancreatitis is a less likely differential.
The patient was discussed in an MDM and referred for EUS and further CT Pancreas.


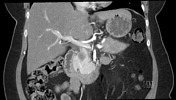


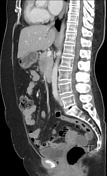
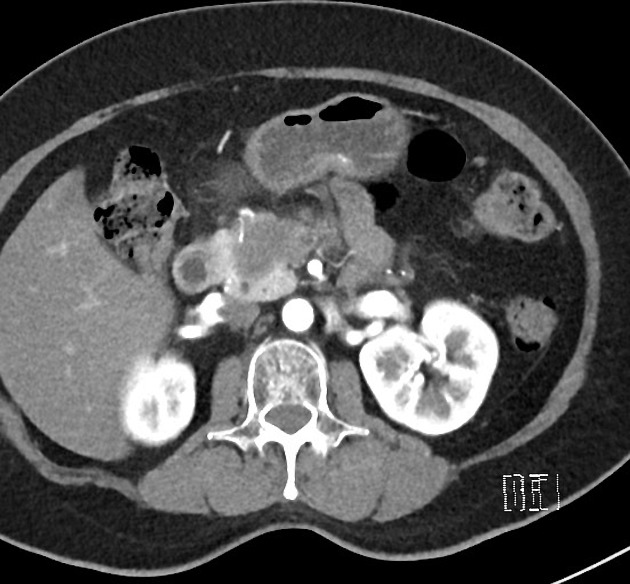
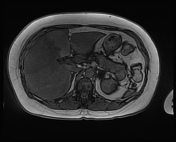
There is a 3 x 2 cm pancreatic head mass which demonstrates slow progressive enhancement, hypoenhancing relative to the remainder of the pancreas. There is only minimal upstream main duct prominence with an abrupt cut-off as seen on recent MRCP. No pancreatic calcifications. There is no evidence of biliary obstruction.
The mass extends inferiorly into the small bowel mesentery. There is a focal severe narrowing of the SMV. There is SMV abutment over a distance of 42 mm. There is portal vein abutment of a distance of 25 mm. There is a first and second jejunal branch involvement.
Celiac axis, hepatic artery, and superior mesenteric artery are clear. GDA is encased.
Small nodules are shown in the small bowel mesentery, measuring 4 mm. No other abnormal lymph nodes by size or appearance in the abdomen or pelvis.
There is geographical, diffuse fatty infiltration of the liver. No liver metastasis. There is a lipid-rich left adrenal adenoma measuring 20 mm. This is not a metastasis. The right adrenal gland is normal.
Focal right renal scarring. Small cortical renal cysts. No solid renal mass. The spleen is normal in appearance. No free fluid. Small and large bowel appear unremarkable.
The visible bones are normal in appearance. Degenerative lumbosacral junction.
Macroscopy: Endoscopic ultrasound-guided FNA of pancreatic head mass - 3 passes: 2 air-dried and 2 alcohol-fixed smears prepared. Cytologist in attendance. Cellblock prepared.
Microscopy: The smears show a population of atypical epithelial cells arranged in variably sized sheets and papillary fragments, exhibiting enlarged, hyperchromatic, pleomorphic nuclei, increased nuclear to cytoplasmic ratios, irregularities of nuclear membranes, coarsening of nuclear chromatin, macronucleoli and moderate amounts of vacuolated cytoplasm. Benign ductal and acinar epithelium are present within the blood-stained background.
Conclusion: Pancreatic head mass, endoscopic ultrasound-guided FNA: Malignant. Features consistent with adenocarcinoma.
Case Discussion
Imaging features of pancreatic head adenocarcinoma that is anatomically borderline resectable with SMV and jejunal branch involvement.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.