
Presentation
Chest pain and difficulty of breathing.
Patient Data


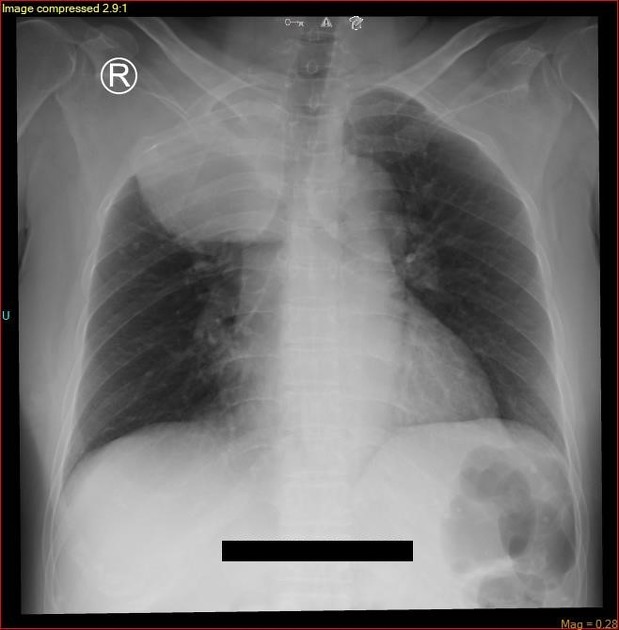
Initial chest radiograph (image 1) in supine position shows a large mass-like convex soft tissue opacity in the right superior posterior mediastinum.
Follow-up radiograph (image 2) taken few days after in upright position however revealed a lobulated mass-like structure in the right hilar region. No surgical intervention was performed in the interim.
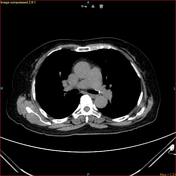




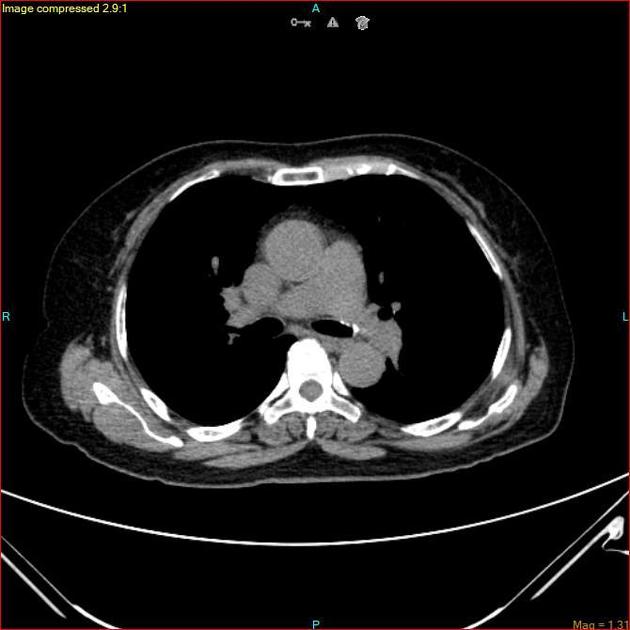
Contrast-enhanced CT of the chest shows a large aneurysmal vessel above the right tracheobronchial angle mildly compressing and draining into the superior vena cava (T5 vertebra level). Within the aneurysm is thrombus extending to the SVC and expanding the azygocaval junction. Multifocal filling defects are noted in the right upper lobe, lingula and left lower lobe representing segmental and subsegmental pulmonary thromboembolism.
Case Discussion
The superior border of the large mass-like opacity in the initial radiograph extends above the right clavicle suggesting its location in the posterior mediastinum (cervicothoracic sign). Its apparent disappearance or migration on follow-up radiograph was due to decrease in the central venous pressure (CVP) observed during upright position allowing blood to drain into the SVC which resulted to the partial collapse of the aneurysm into the right hilar region. Change in size and shape, upon maneuvers which alters the CVP, is a characteristic known to intrathoracic venous aneurysms.
Similar to the aneurysmal vessel identified on chest CT, the azygos vein arches over the right mainstem bronchus from the posterior mediastinum to drain into the SVC at T5 vertebral level. The azygocaval junction is the confluence of cardinal venous derivatives which serves as an anatomic weak-point leading to development of aneurysm. Azygos vein aneurysm (AVA) was confirmed on surgery.
AVA in itself is a rare pathology. AVA complicated by intra-aneurysmal thrombosis with secondary pulmonary thromboembolism is even a more rare case.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.