
Presentation
Colicky abdominal pain, nausea and vomiting since 2 days ago
Patient Data
Age: 80 years
Gender: Male
From the case:
Small bowel obstruction - bezoar



Download
Info
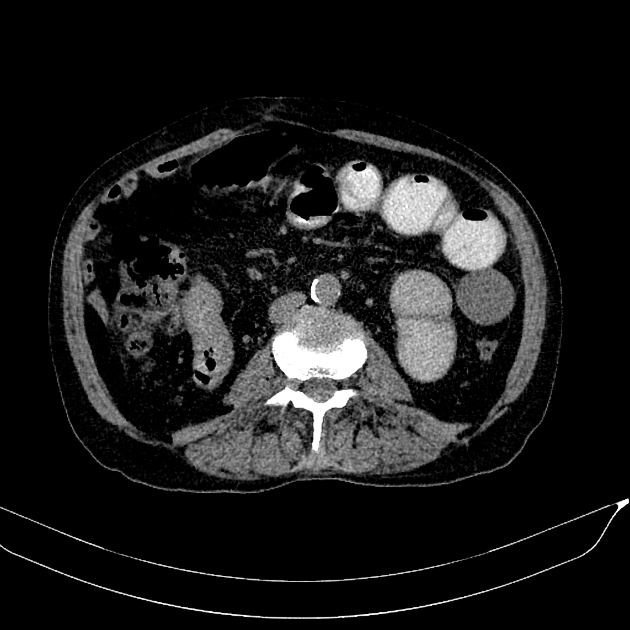
Dilated proximal two-third of small bowel loops with the collapsed distal ileal loop is seen in favor of partial mechanical obstruction. A porous intraluminal oval filling defect (red arrow) is seen just before the transitional zone in favor of bezoar as the cause. No sign of close loop formation, strangulation or perforation is still detected.
Case Discussion
Patient underwent conservative management and obstruction signs were resolved after the CT scan. Resolution of partial obstruction after CT scan with ingestion of oral contrast agent is common because of osmotic pressure created by the ingested contrast agent.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.