
Presentation
Abdominal pain and dyspepsia.
Patient Data
Age: 45 years
Gender: Female
From the case:
Gastric adenocarcinoma





Download
Info
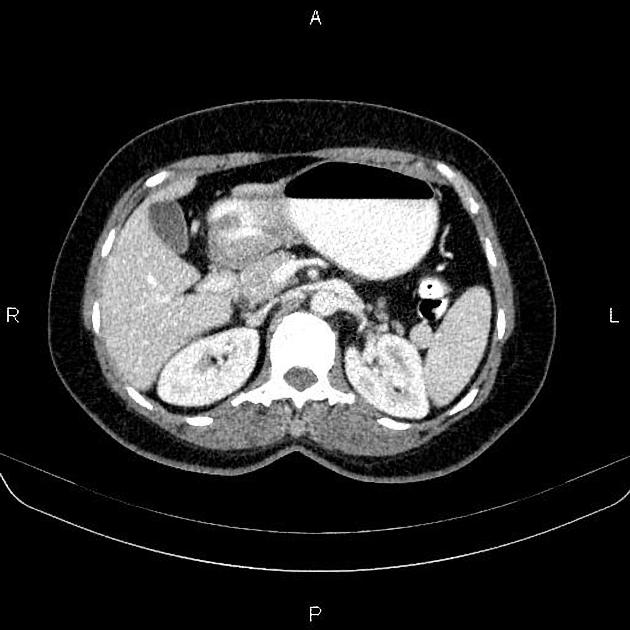
Increased wall thickness as tumoral infiltration is present at gastric antrum. No local invasion to adjacent structures and no obvious regional lymphadenopathy are noted.
Mild degenerative changes as osteophytosis is seen at the lumbar spine.
Case Discussion
Pathologically-proven gastric antral adenocarcinoma which is the most common gastric malignancy and the third most common GI malignancy following colon and pancreatic carcinoma.
CT is currently the staging modality of choice because it can help identify the primary tumor, assess for local spread, detect nodal involvement and distant metastases.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.