
Presentation
Abdominal pain and dyspepsia.
Patient Data






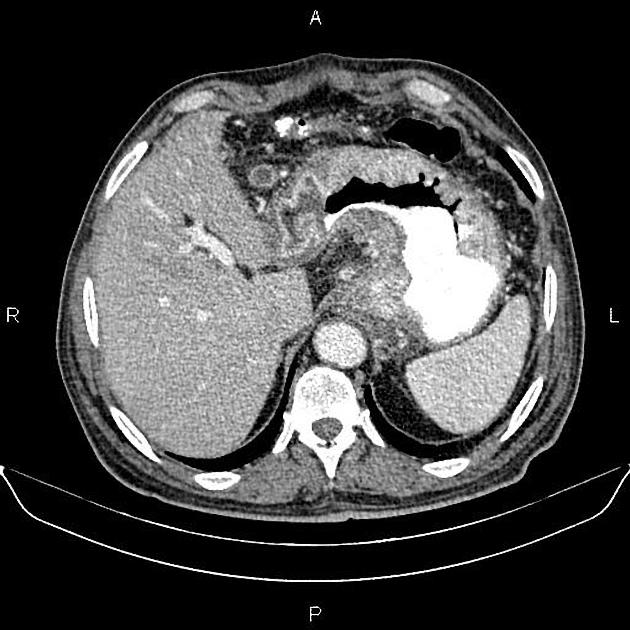
Marked increased wall thickness due to tumoral infiltration is present at esophagogastric junction, gastric cardia and body accompanied by adjacent fat stranding.
Multiple lymphadenopathies with SAD less than 20 mm are noted in the vicinity of diseased segment. There is no sign of local invasion to adjacent structures.
A 70 mm simple cortical cyst is present at left kidney.
The prostate gland is enlarged.
Degenerative changes as osteophytosis are seen at the thoracolumbar spine.
Grade I spondylolisthesis of L5 on S1 is present with bilateral spondylolysis.
Case Discussion
Patient underwent total gastrectomy and esophagojejunostomy.
PATHOLOGY REPORT:
Adenocarcinoma, intestinal type, poorly differentiated.
ICD diagnosis code:M140/3 C16.9


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.