
Presentation
Recurrent episodes of abdominal pain radiating to both flanks, associated with fever, vomiting, and anorexia. Elevated pancreatic enzymes suspected pancreatitis.
Patient Data
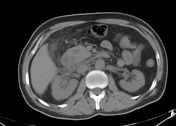



The head of pancreas appears thickened along with wall thickening of the second part of the duodenum followed by stenosis. Free fluid and fatty stranding are seen mainly in the pancreaticoduodenal groove extending into anterior pararenal space.
Thickening of the Gerota fascia is seen and small amount of fluid is seen extending also in the right infrarenal space.
Dilated common bile duct is also noted.
No evidence of calcifications involving the pancreas, and the pancreatic body and tail appearances unremarkable.
No evidence of free gas or lymph node enlargement could be seen.
Findings are highly suggestive of focal pancreatitis affecting mainly its head and duodenitis.
The liver and spleen are normal in size and have homogenous texture without evidence of focal lesion.
The spleen, adrenal glands, and kidneys appear normal.



In addition to features of Paraduodenal pancreatitis the head of pancreas is thickened and appears hypodense.
Later developed, bilateral pleural effusion more on the right side with basal atelectasis.

Arrow points towards the pancreaticoduodenal groove.
Case Discussion
CT features are most consistent with Paraduodenal pancreatitis (A.K.A groove pancreatitis). It is an uncommon type of chronic focal pancreatitis affecting the groove between the head of the pancreas, the duodenum, and the common bile duct. The duodenum is always involved with scar tissue in the wall leading to fibrosis and various levels of stenosis.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.