
Presentation
Routine first trimester scan.
Patient Data
Both kidneys are average in size with mild echogenic echopattern.
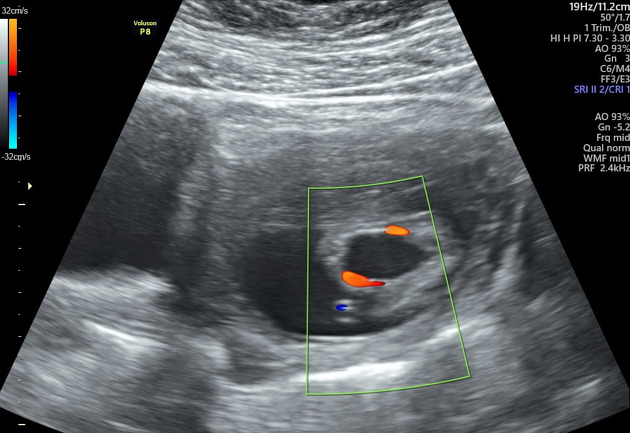
Distended urinary bladder (megacystis) with tapered bladder neck by the ectatic posterior urethra, suggestive of bladder outlet obstruction.
Mild fetal bradycardia is noted (FHR=125 b/min).
Increased nuchal translucency thickness (2.6 mm).

The kidneys are normal in size with preserved reniform shape with highly echogenic cortices, loss of cortico-medullary differentiation and mild symmetrical pelvicalyceal dilatation.
Mild fetal bradycardia is still noted (FHR=122 b/min).
The urinary bladder shows more distension (24 x 18 mm in axial diameters), and craniocaudal dimension of approx. 29 mm, with tapered appearance of the bladder neck consistent with bladder outlet obstruction.
Oligohydramnios is noted (AFI=4.5)

Empty urinary bladder at the time of examination, consistent with resolved megacystis.
Increased echogenicity of both kidneys, currently mild echogenic.
Residual dilatation of both renal pelvises (pyelectasis) with no impression of current obstruction.
- right renal pelvis AP diameter = 4 mm
- left renal pelvis AP diameter = 4.9 mm
Normal size of both kidneys for gestational age averaging 2 x 1 cm.
Regained normal amniotic fluid volume (AFI=13.5 – single pocket = 5 cm)
Fetal gestational age matches with the EDD based on LMP revealing normal growth pattern.
Case Discussion
Follow up study revealed progressive urinary obstruction with the development of mild bilateral hydronephrosis and progressive increased renal echogenicity.
The presence of oligohydramnios is in keeping with urinary bladder outflow obstruction. The echogenic kidneys in the presence of obstruction is suggestive of obstructive cystic renal dysplasia as a result of urinary obstruction. The possible cause, in this case, would be posterior urethral valve. Amniocentesis is advised in this case, as this case has high association with chromosomal anomalies.
If the urinary bladder is small + bilateral echogenic kidneys + oligohydramnios, we would suggest autosomal recessive polycystic kidney disease (ARPCKD) and Finnish type congenital nephrotic syndrome.
Fortunately, on follow up 20 weeks scan the urinary bladder was seen empty during the examination, which means megacystis has resolved. Only residual pyelectasis seen. It was reported that fetal megacystis can resolve spontaneously before 23rd week 1.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.