
Presentation
Abdominal pain and dyspepsia.
Patient Data






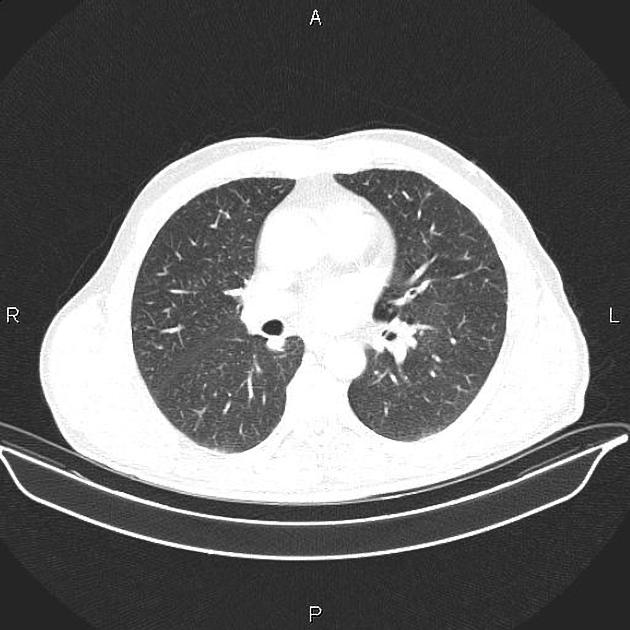
Subpleural fibrotic changes and honeycombing are seen at both upper lobes. Additionally, A few small nodules, less than 4 mm are scattered at both lungs which seems to be fibrotic nodules.
Marked increased wall thickness due to tumoral infiltration is present at gastric body and antrum accompanied by several regional lymphadenopathies with maximum SAD of 30 mm. Fat plane between the mass and pancreas is preserved.
Several non-enhanced simple cortical cysts are seen at both kidneys.
Case Discussion
Pathology proven case of gastric adenocarcinoma with regional lymphadenopathy.
CT is currently the staging modality of choice because it can help identify the primary tumor, assess for the local spread, and detect nodal involvement and distant metastases.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.