
Presentation
Progressive abdominal distension and elevated liver enzymes.
Patient Data


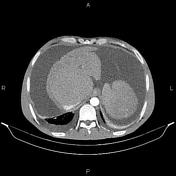

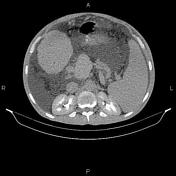


Massive abdominopelvic ascites is present.
The liver shows coarse parenchyma and irregular margin with marked caudate lobe enlargement in keeping with cirrhosis. No obvious hypervascular hepatic mass in current study to suggest HCC. Some collateral vessels are seen at perihepatic regions.
Multiple hyperdense stones are seen at gallbladder less than 18mm.
The spleen is enlarged and its cephalocaudal height measured 210mm.
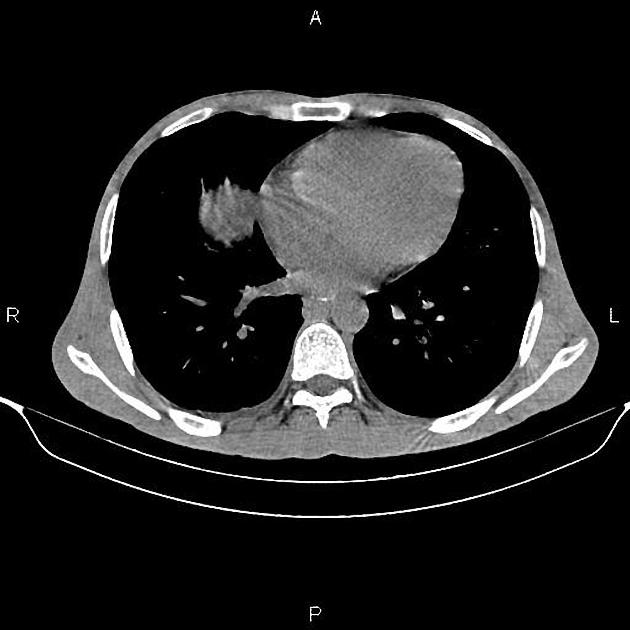
The right subclavian artery is arising from the arch of aorta directly posterior to the esophagus inferring aberrant right subclavian artery.
A little amount pleural effusion is present bilaterally.
Case Discussion
Cirrhosis with evidence of portal hypertension, splenomegaly and massive ascites.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.