
Presentation
Left flank pain and fullness.
Patient Data
Age: 30 years
Gender: Male
From the case:
Renal cell carcinoma





Download
Info
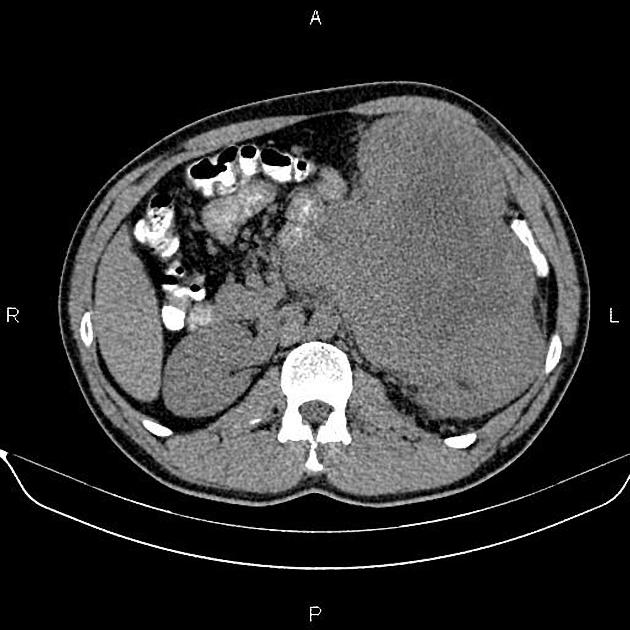
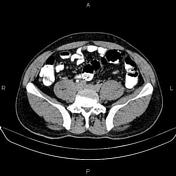
Huge heteroenhancing mass with lobulated margin is present at left kidney measuring 190×150×170 mm in diameters. Fat planes between the mass and left psoas muscle are obliterated is some areas. There is no frank sign of local invasion into other adjacent organs. Left renal vein is obliterated and left renal artery seems to partially encased by the mass.
Several small lymphadenopathies are noted at left paraaortic regions with SAD less than 8 mm.
Case Discussion
Huge left renal mass; pathology proven renal cell carcinoma (clear cell subtype) with local invasion to psoas muscle, vascular involvement and para-aortic lymphadenopathies.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.