
Presentation
Nasal congestion.
Patient Data
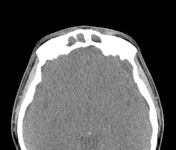



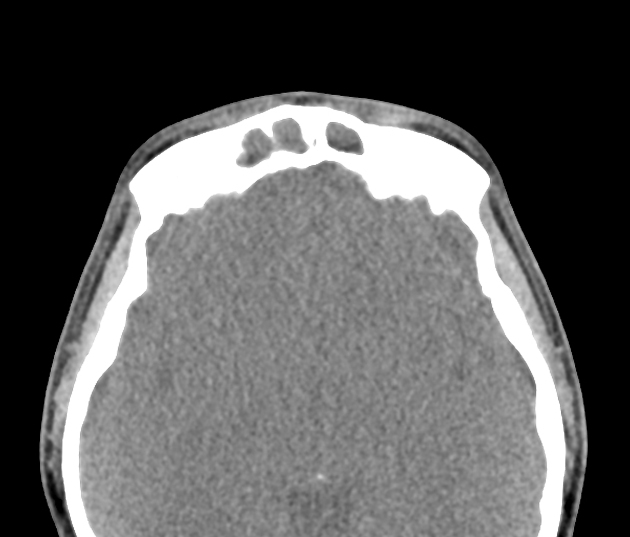
Extensive paranasal sinus and mastoid air cell opacification.
Erosion of the medial walls of the maxillary sinuses and nasal turbinates.
Complete opacification of the mastoid air cells.


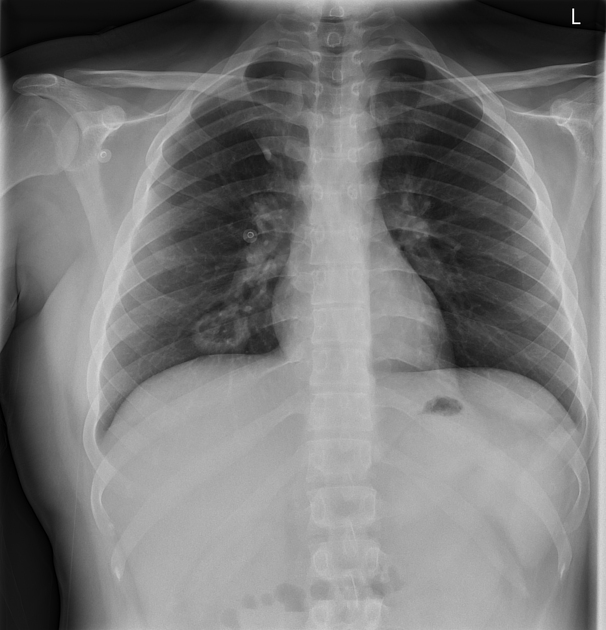
4 cm ovoid cavitating lesion in the right middle lobe, with air-fluid level.
Lungs otherwise clear.
Normal cardiomediastinal contour.




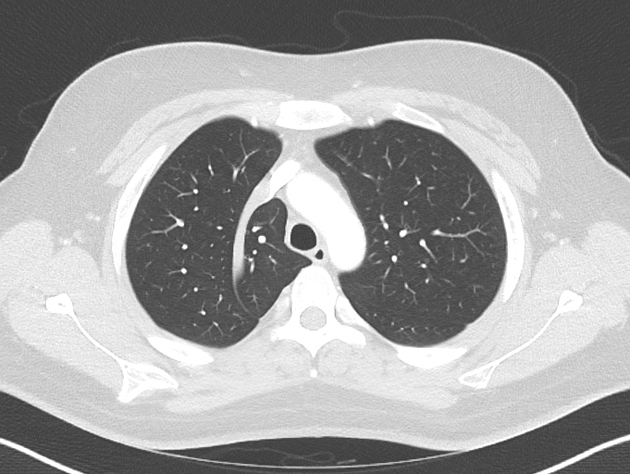
Solitary, irregular and thick walled cavitating lesion with air-fluid level in the right middle lobe, measuring 3 x 3.5 x 2.5 cm.
Extensive ill-defined soft tissue thickening around the right central bronchi and right main bronchus tracking up to the carina, causing luminal irregularity.
No pulmonary collapse.
Lungs and pleural spaces are otherwise clear. Incidental azygos fissure.
Filling defects in bilateral lower lobe segmental and subsegmental pulmonary arteries.
No evidence of right heart strain.
No lymphadenopathy.
No destructive osseous lesion identified.
Case Discussion
According to the 1990 American College of Rheumatology criteria, two of the following are required for a diagnosis of granulomatosis with polyangiitis to be made:
- positive biopsy for granulomatous vasculitis
- urinary sediment with red blood cells
- abnormal chest radiograph
- oral or nasal inflammation
The classic triad of organ involvement consists of:
- lungs: involved in ~95% of cases
- upper respiratory tract / sinuses: ~75-90%
- kidneys: ~80%


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.