
Presentation
Abdominal pain.
Patient Data




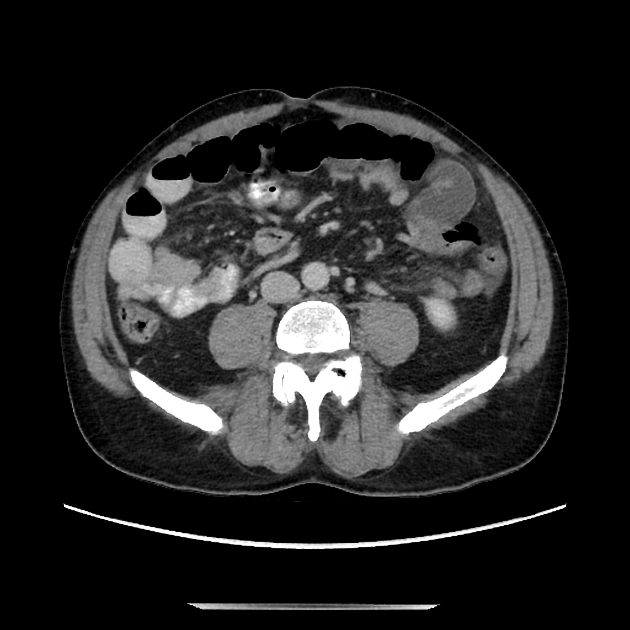
Mild dilation of a few loops of mid small bowel which transition into sharp narrowing in the left mid abdomen, leading into a cluster of non-dilated but radially oriented (see coronal images) small bowel with mesenteric edema. This cluster transitions back to normal decompressed distal small bowel next to the entrance, indicating a closed loop (this is best seen on the axial images).
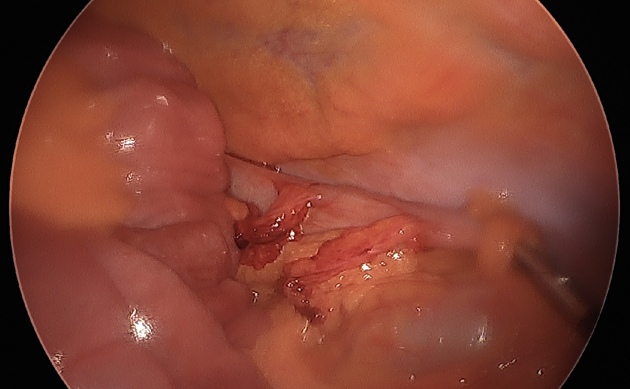
Intraoperative image of entrance of the internal hernia.
Case Discussion
This is a case of surgically-confirmed closed loop obstruction/physiology due to an internal hernia, which did not require small bowel resection as the bowel was mildly erythematous and edematous but not ischemic. The internal hernia was found to be conjoined dual colonic epiploica, which formed the defect through which the small bowel cluster "fell into". Note that the closed loop is not actually dilated, but rather relatively decompressed, but you can identify it because of the asymmetric mesenteric edema and radial orientation on the coronal images. The axial images are best for following the mildly dilated small bowel into and out of the closed loop, and on those images you can see both transition points next to each other.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.