
Presentation
Fall onto the outstretched hand while playing. Kirmisson sign upon physical examination.
Patient Data
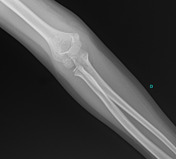


Elbow radiographs revealed a supracondylar humeral fracture. The lateral projection shows posterior displacement, and an anterior cortical disruption with an intact posterior cortex, in keeping with a Gartland type II fracture.
No fracture lines were seen on the frontal projection.
Moderate elbow joint effusion is noted by the sail sign and posterior fat pad sign.
(See annotated images below)

The anterior humeral line was assessed and identified as not intersecting the capitellum. This indicates a displaced supracondylar fracture.

White arrowheads pointing to the elbow joint effusion. The anterior fat pad has a triangular appearance in keeping with the sail sign. The posterior fat pad is seen, which it normally would not be.
Case Discussion
Supracondylar fractures are the most common elbow fractures in children. Fall onto the outstretched hand with the elbow in full extension is the main mechanism of injury.
Gartland type II fractures are displaced (>2 mm) supracondylar fractures with an intact posterior cortex.
In the present case, there was moderate elbow joint effusion, noticeable by the sail sign and posterior fat pad sign, which is common for supracondylar fracture. Also, the anterior humeral line was not passing through the capitellum, which indicates a displaced fracture.
Finally, it's important to be familiar with the elbow ossification centers when assessing a pediatric elbow. In this case, only the capitellum and radial head ossification centers are visible, which is normal given the patient's age.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.